

Hyaluronic Acid Hydrogel Integrated with Mesenchymal Stem Cell-Secretome to Treat Endometrial Injury in a Rat Model of Asherman's Syndrome
- PMID: 31148407
- PMCID: PMC7045702
- DOI: 10.1002/adhm.201900411
Hyaluronic Acid Hydrogel Integrated with Mesenchymal Stem Cell-Secretome to Treat Endometrial Injury in a Rat Model of Asherman's Syndrome
Abstract
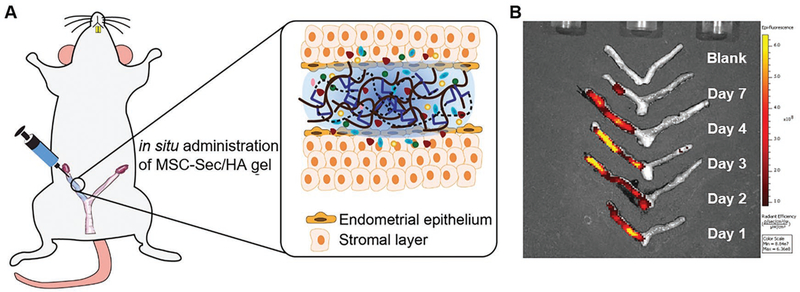
Stem cell therapies have made strides toward the efficacious treatment of injured endometrium and the prevention of intrauterine adhesions, or Asherman's syndrome (AS). Despite this progress, they are limited by their risk of tumor formation, low engraftment rates, as well as storage and transportation logistics. While attempts have been made to curb these issues, there remains a need for simple and effective solutions. A growing body of evidence supports the theory that delivering media, conditioned with mesenchymal stem cells, might be a promising alternative to live cell therapy. Mesenchymal stem cell-secretome (MSC-Sec) has a superior safety profile and can be stored without losing its regenerative properties. It is versatile enough to be added to a number of delivery vehicles that improve engraftment and control the release of the therapeutic. Thus, it holds great potential for the treatment of AS. Here, a new strategy for loading crosslinked hyaluronic acid gel (HA gel) with MSC-Sec is reported. The HA gel/MSC-Sec treatment paradigm creates a sustained release system that repairs endometrial injury in rats and promotes viable pregnancy.
Keywords: Asherman's syndrome; endometrial injury; hyaluronic acid; mesenchymal stem cells; secretome.
© 2019 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim.
Conflict of interest statement
Conflict of Interest
The authors declare no conflict of interest.
Figures
References
-
- Hooker AB, Lemmers M, Thurkow AL, Heymans MW, Opmeer BC, Brolmann HA, Mol BW, Huirne JA, Hum. Reprod. Update 2014, 20, 262. - PubMed
-
- Berman JM, Semin. Reprod. Med. 2008, 26, 349. - PubMed
-
- Chen L, Zhang H, Wang Q, Xie F, Gao S, Song Y, Dong J, Feng H, Xie K, Sui L, J. Minimally Invasive Gynecol. 2017, 24, 299. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
