

Effect of ferric carboxymaltose on calculated plasma volume status and clinical congestion: a FAIR-HF substudy
- PMID: 31148411
- PMCID: PMC6676445
- DOI: 10.1002/ehf2.12462
Effect of ferric carboxymaltose on calculated plasma volume status and clinical congestion: a FAIR-HF substudy
Abstract
Aims: Iron deficiency worsens symptoms, quality of life, and exercise capacity in chronic heart failure (CHF) and might do so by promoting fluid retention. We assessed whether iron repletion improved congestion in CHF and appraised the prognostic utility of calculated plasma volume status (PVS), a novel index of congestion, in the FAIR-HF data set.
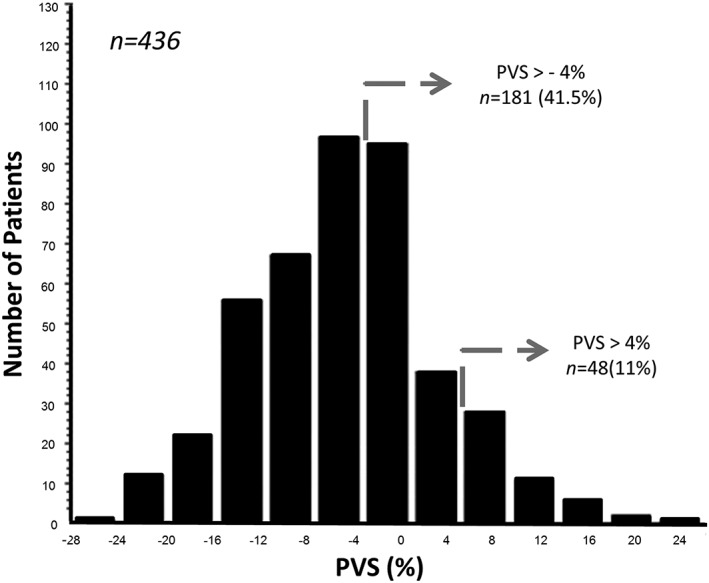
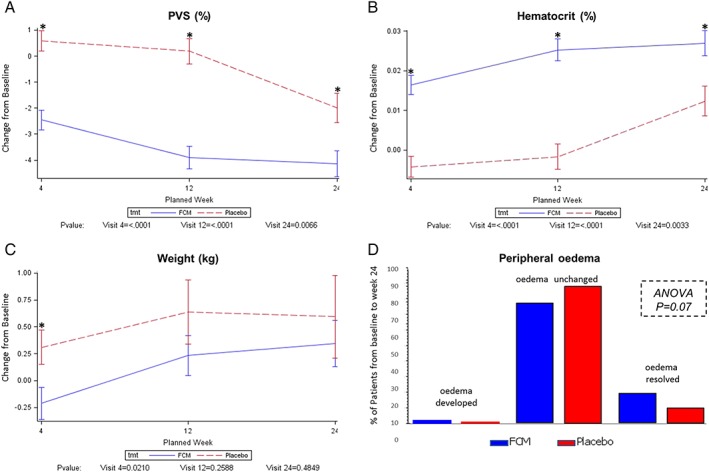
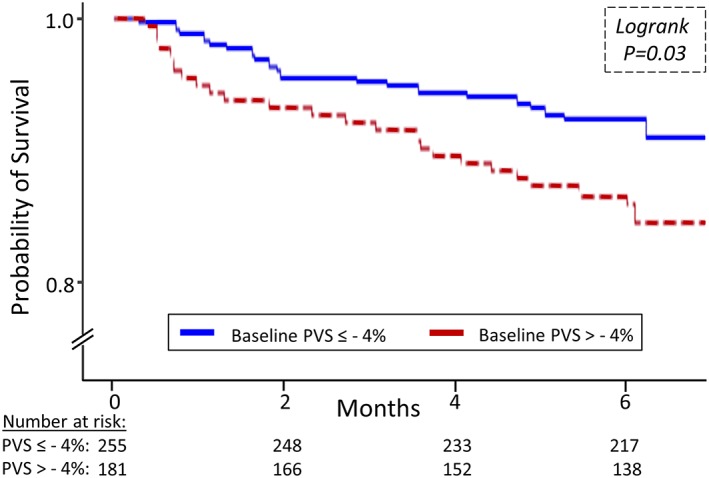
Methods and results: In FAIR-HF, 459 iron deficient CHF patients were randomized to intravenous ferric carboxymaltose (FCM) or saline and assessed at 4, 12, and 24 weeks. Using weight and haematocrit, we calculated PVS in 436 patients. At baseline, PVS and weight were -5.5 ± 7.7% and 76.9 ± 14.3 kg, with peripheral oedema evident in 35% of subjects. Higher PVS values correlated to other congestion surrogates such as lower serum albumin. At 4 weeks, FCM was associated with greater reductions in weight (0.02) and PVS (P < 0.0001), and a trend for improved peripheral oedema at 24 weeks (0.07). Irrespective of treatment allocation, patients with a decrease in PVS from baseline to week 24 had higher increments in 6 min walking distance (61.4 m vs. 43.5 m, 0.02) and were more likely to improve their NYHA class (33.3% vs. 15.5%, 0.001). A PVS > -4% at baseline predicted worse outcomes even after adjustment for treatment assignment (hazard ratio 1.88, 95% confidence interval 1.01-3.51, 0.046).
Conclusions: Intravenous iron therapy with FCM is associated with early reductions in PVS and weight, implying that decongestion might be one mechanism via which iron repletion aids CHF patients. Calculated PVS is of prognostic utility in this cohort.
Keywords: Congestion; Iron; Oedema; Plasma volume.
© 2019 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
The FAIR‐HF trial was supported by Vifor Pharma, Glattbrugg, Switzerland. All authors had full access to the study data, decided to submit the report for publication, and assume responsibility for the completeness and accuracy of the data, and the content and integrity of the report. C.M. and S.C. are employees of Vifor. D.O.O. has received speaker's fees and research support from Vifor and Pharmacosmos. S.D.A. has received fees for consulting and/or speaking from Bayer, Boehringer Ingelheim, Novartis, Servier, and Vifor. S.D.A. has received research grants from Abbott Vascular and Vifor. G.P. is a member of Committees in trials and registries sponsored by Vifor, Novartis, Bayer, and Servier. P.P. has received consulting and speaker's fees and research grants from Vifor.
Figures
References
-
- Okonko DO, Mandal AK, Missouris CG, Poole‐Wilson PA. Disordered iron homeostasis in chronic heart failure: prevalence, predictors and relation to anemia, exercise capacity and survival. J Am Coll Cardiol 2011; 58: 1241–1251. - PubMed
-
- Jankowska EA, Tkaczyszyn M, Suchocki T, Droz D, von Haehling S, Doehner W, Banasiak W, Filippatos G, Anker SD, Ponikowski P. Effects of intravenous iron therapy in iron‐deficient patients with systolic heart failure: a meta‐analysis of randomised controlled trials. Eur J Heart Fail 2016; 18: 786–795. - PubMed
-
- Nunez J, Comin‐Colet J, Minana G, Nunez E, Santas E, Mollar A, Valero E, Garcia‐Blas S, Cardells I, Bodi V, Chorro FJ, Sanchis J. Iron deficiency and risk of early readmission following a hospitalization for heart failure. Eur J Heart Fail 2016; 18: 798–802. - PubMed
-
- Dupont M, Mullens W, Tang WH. Impact of systemic venous congestion in heart failure. Curr Heart Fail Rep 2011; 8: 233–241. - PubMed
-
- Klein L. Treating hemodynamic congestion is the key to prevent heart failure hospitalizations. JACC Heart Fail 2016; 4: 345–347. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
