

Factors influencing glycaemic stability after neonatal hypoglycaemia and relationship to neurodevelopmental outcome
- PMID: 31148566
- PMCID: PMC6544629
- DOI: 10.1038/s41598-019-44609-1
Factors influencing glycaemic stability after neonatal hypoglycaemia and relationship to neurodevelopmental outcome
Abstract
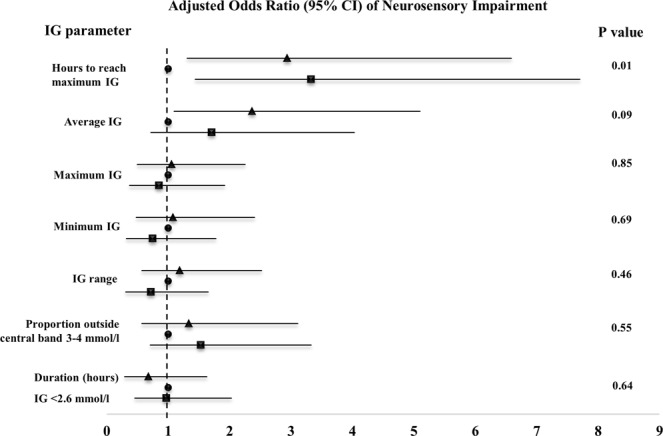
Higher and unstable glucose concentrations in the first 48 hours in neonates at risk of hypoglycaemia have been associated with neurosensory impairment. It is unclear what defines and contributes to instability. This was a prospective study of term and late preterm babies (N = 139) born at risk of neonatal hypoglycaemia who had interstitial glucose (IG) monitoring and ≥1 hypoglycaemic episode <48 hours after birth (blood glucose concentration <2.6 mmol/l [<47 mg/dl]). For 6-hour epochs after each hypoglycaemic episode, masked IG parameters (time to reach maximum IG concentration [hours]; range, average, maximum and minimum IG concentrations; proportion of IG measurements outside the central band of 3-4 mmol/l [54-72 md/dl]; and total duration [hours] of IG concentrations <2.6 mmol/l) were analysed in tertiles and related to: (i) glycaemic instability in the first 48 hours (defined as the proportion of blood glucose concentrations outside the central band in the first 48 hours); (ii) risk factors and treatment for each episode; and (iii) risk of neurosensory impairment at 4.5 years, or at 2 years if a child was not seen at 4.5 years. Glycaemic instability in the first 48 hours was related to IG instability after hypoglycaemia. Risk factors for hypoglycaemia were not related to IG parameters. Treatment with intravenous dextrose was associated with higher IG maximum and range, and lower minimum compared to treatment with dextrose gel plus breast milk, breast milk alone or formula alone. The risk of neurosensory impairment was increased with both shorter and longer time to reach maximum epoch IG (P = 0.04; lower tertile [0.4-2.2 hours] vs middle [2.3-4.2 hours] OR 3.10 [95% CI 1.03; 9.38]; higher tertile [4.3-6.0 hours] vs middle OR 3.07; [95% CI 1.01; 9.24]). Glycaemic response to hypoglycaemia contributes to overall glycaemic instability in newborns and is influenced by treatment. Slow or rapid recovery of hypoglycaemia appears to be associated with neurosensory impairment.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Hawdon JM. Investigation, prevention and management of neonatal hypoglycaemia (impaired postnatal metabolic adaptation) Paediatr Child Health (GBR). 2012;22:131–135. doi: 10.1016/j.paed.2011.08.006. - DOI
-
- Hawdon JM. Investigation and management of impaired metabolic adaptation presenting as neonatal hypoglycaemia. Paediatr Child Health (GBR). 2008;8:161–165. doi: 10.1016/j.paed.2007.12.012. - DOI
-
- Hawdon JM. Postnatal metabolic adaptation and neonatal hypoglycaemia. Paediatr Child Health. 2016;26:135–139. doi: 10.1016/j.paed.2015.12.001. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
