

The Occupational Burden of Nonmalignant Respiratory Diseases. An Official American Thoracic Society and European Respiratory Society Statement
- PMID: 31149852
- PMCID: PMC6543721
- DOI: 10.1164/rccm.201904-0717ST
The Occupational Burden of Nonmalignant Respiratory Diseases. An Official American Thoracic Society and European Respiratory Society Statement
Abstract
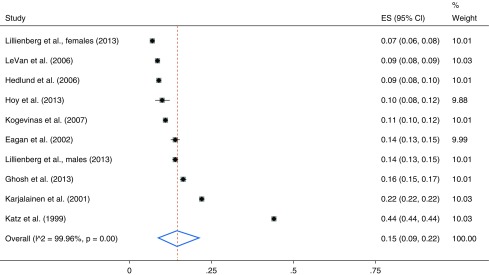
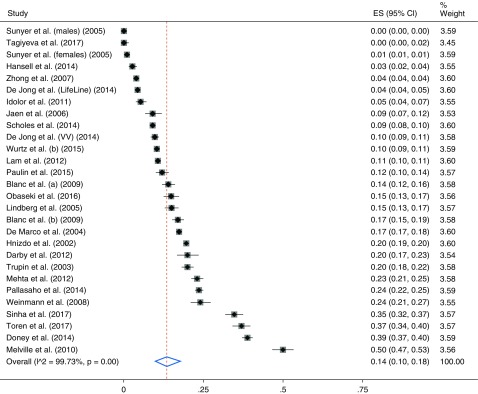
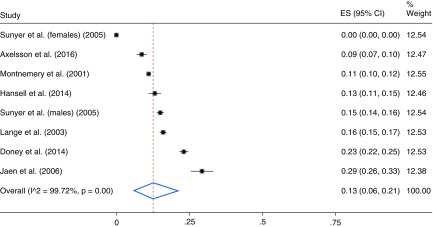
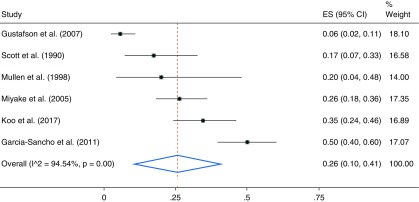
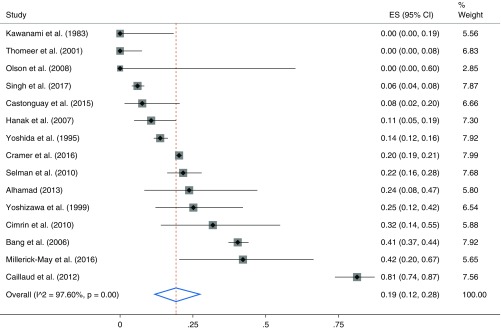
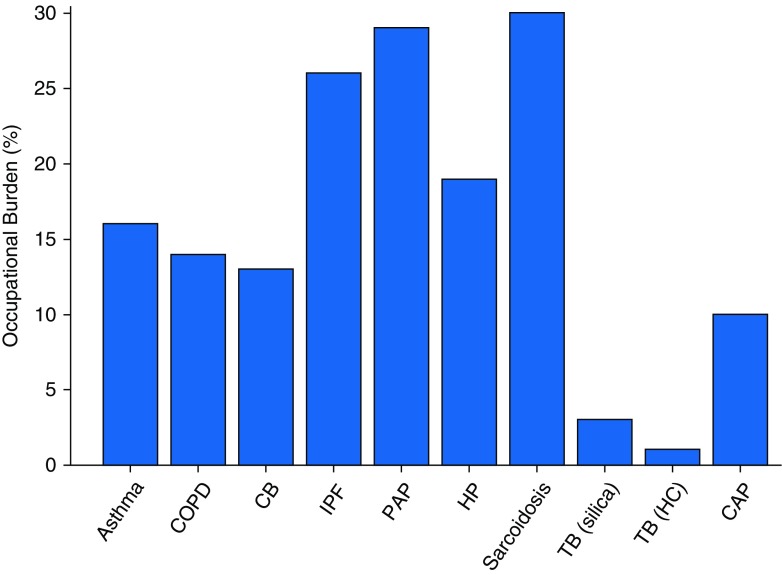
Rationale: Workplace inhalational hazards remain common worldwide, even though they are ameliorable. Previous American Thoracic Society documents have assessed the contribution of workplace exposures to asthma and chronic obstructive pulmonary disease on a population level, but not to other chronic respiratory diseases. The goal of this document is to report an in-depth literature review and data synthesis of the occupational contribution to the burden of the major nonmalignant respiratory diseases, including airway diseases; interstitial fibrosis; hypersensitivity pneumonitis; other noninfectious granulomatous lung diseases, including sarcoidosis; and selected respiratory infections. Methods: Relevant literature was identified for each respiratory condition. The occupational population attributable fraction (PAF) was estimated for those conditions for which there were sufficient population-based studies to allow pooled estimates. For the other conditions, the occupational burden of disease was estimated on the basis of attribution in case series, incidence rate ratios, or attributable fraction within an exposed group. Results: Workplace exposures contribute substantially to the burden of multiple chronic respiratory diseases, including asthma (PAF, 16%); chronic obstructive pulmonary disease (PAF, 14%); chronic bronchitis (PAF, 13%); idiopathic pulmonary fibrosis (PAF, 26%); hypersensitivity pneumonitis (occupational burden, 19%); other granulomatous diseases, including sarcoidosis (occupational burden, 30%); pulmonary alveolar proteinosis (occupational burden, 29%); tuberculosis (occupational burden, 2.3% in silica-exposed workers and 1% in healthcare workers); and community-acquired pneumonia in working-age adults (PAF, 10%). Conclusions: Workplace exposures contribute to the burden of disease across a range of nonmalignant lung conditions in adults (in addition to the 100% burden for the classic occupational pneumoconioses). This burden has important clinical, research, and policy implications. There is a pressing need to improve clinical recognition and public health awareness of the contribution of occupational factors across a range of nonmalignant respiratory diseases.
Keywords: interstitial fibrosis; nonmalignant respiratory diseases; occupational; pneumonitis; respiratory infections; sarcoidosis; workplace.
Figures
Comment in
-
Occupational Burden in Chronic Respiratory Disease: Call for Recognition, Training, and Data Capture.Am J Respir Crit Care Med. 2019 Dec 15;200(12):1558-1559. doi: 10.1164/rccm.201907-1288LE. Am J Respir Crit Care Med. 2019. PMID: 31343258 Free PMC article. No abstract available.
-
Reply to Lee and Strek: Occupational Burden in Chronic Respiratory Disease: Call for Recognition, Training, and Data Capture.Am J Respir Crit Care Med. 2019 Dec 15;200(12):1559. doi: 10.1164/rccm.201907-1379LE. Am J Respir Crit Care Med. 2019. PMID: 31343269 Free PMC article. No abstract available.
References
-
- Driscoll T, Nelson DI, Steenland K, Leigh J, Concha-Barrientos M, Fingerhut M, et al. The global burden of non-malignant respiratory disease due to occupational airborne exposures. Am J Ind Med. 2005;48:432–445. - PubMed
-
- Balmes J, Becklake M, Blanc P, Henneberger P, Kreiss K, Mapp C, et al. Environmental and Occupational Health Assembly, American Thoracic Societ. American Thoracic Society statement: occupational contribution to the burden of airway disease. Am J Respir Crit Care Med. 2003;167:787–797. - PubMed
-
- Eisner MD, Anthonisen N, Coultas D, Kuenzli N, Perez-Padilla R, Postma D, et al. Committee on Nonsmoking COPD, Environmental and Occupational Health Assembly. An official American Thoracic Society public policy statement: novel risk factors and the global burden of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2010;182:693–718. - PubMed
-
- Henneberger PK, Redlich CA, Callahan DB, Harber P, Lemière C, Martin J, et al. ATS Ad Hoc Committee on Work-Exacerbated Asthma. An official American Thoracic Society statement: work-exacerbated asthma. Am J Respir Crit Care Med. 2011;184:368–378. - PubMed
-
- Taskar VS, Coultas DB. Is idiopathic pulmonary fibrosis an environmental disease? Proc Am Thorac Soc. 2006;3:293–298. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
