

Early warning systems in obstetrics: A systematic literature review
- PMID: 31150513
- PMCID: PMC6544303
- DOI: 10.1371/journal.pone.0217864
Early warning systems in obstetrics: A systematic literature review
Abstract
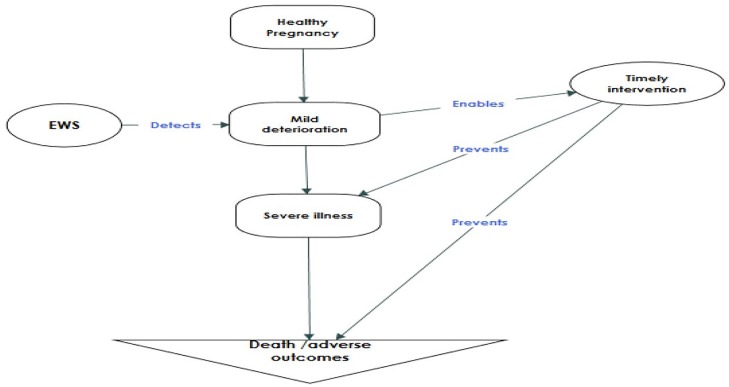
Introduction: Several versions of Early Warning Systems (EWS) are used in obstetrics to detect and treat early clinical deterioration to avert morbidity and mortality. EWS can potentially be useful to improve the quality of care and reduce the risk of maternal mortality in resource-limited settings. We conducted a systematic literature review of published obstetric early warning systems, define their predictive accuracy for morbidity and mortality, and their effectiveness in triggering corrective actions and improving health outcomes.
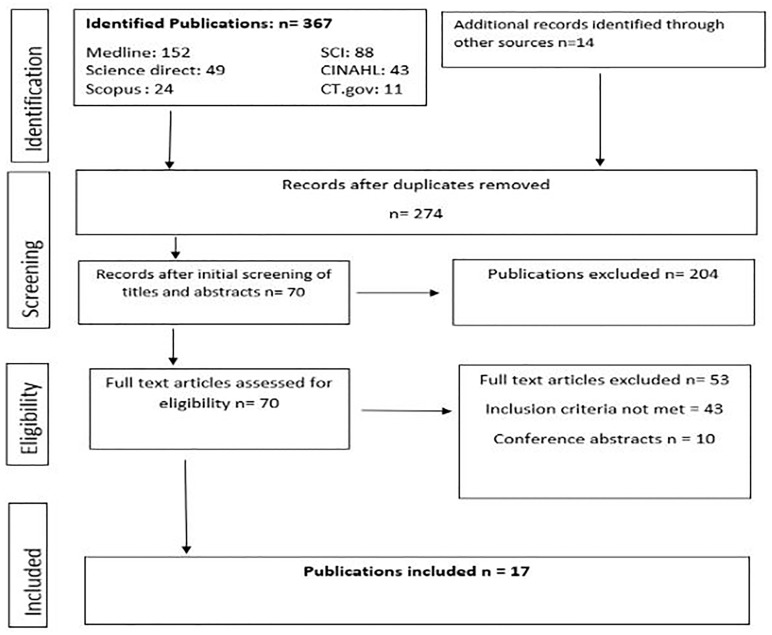
Methods: We systematically searched for primary research articles on obstetric EWS published in peer-reviewed journals between January 1997 and March 2018 in Medline, CINAHL, SCOPUS, Science Direct, and Science Citation Index. We also searched reference lists of relevant articles and websites of professional societies. We included studies that assessed the predictive accuracy of EWS to detect clinical deterioration, or/and their effectiveness in improving clinical outcomes in obstetric inpatients. We excluded studies with a paediatric or non-obstetric adult population. Cross-sectional and qualitative studies were also excluded. We performed a narrative synthesis since the outcomes reported were heterogeneous.
Results: A total of 381 papers were identified, 17 of which met the inclusion criteria. Eleven of the included studies evaluated the predictive accuracy of EWS for obstetric morbidity and mortality, 5 studies assessed the effectiveness of EWS in improving clinical outcomes, while one study addressed both. Sixteen published EWS versions were reviewed, 14 of which included five basic clinical observations (pulse rate, respiratory rate, temperature, blood pressure, and consciousness level). The obstetric EWS identified had very high median (inter-quartile range) sensitivity-89% (72% to 97%) and specificity-85% (67% to 98%) but low median (inter-quartile range) positive predictive values-41% (25% to 74%) for predicting morbidity or ICU admission. Obstetric EWS had a very high accuracy in predicting death (AUROC >0.80) among critically ill obstetric patients. Obstetric EWS improves the frequency of routine vital sign observation, reduces the interval between the recording of specifically defined abnormal clinical observations and corrective clinical actions, and can potentially reduce the severity of obstetric morbidity.
Conclusion: Obstetric EWS are effective in predicting severe morbidity (in general obstetric population) and mortality (in critically ill obstetric patients). EWS can contribute to improved quality of care, prevent progressive obstetric morbidity and improve health outcomes. There is limited evidence of the effectiveness of EWS in reducing maternal death across all settings. Clinical parameters in most obstetric EWS versions are routinely collected in resource-limited settings, therefore implementing EWS may be feasible in such settings.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Alkema L, Chou D, Hogan D, Zhang S, Moller A-B, Gemmill A, et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. Lancet (London, England). Elsevier; 2016;387: 462–74. 10.1016/S0140-6736(15)00838-7 - DOI - PMC - PubMed
-
- Morgan R, Lloyd-Williams F, Wright M, Morgan-Warren R. An early warning scoring system for detecting developing critical illness [Internet]. 1997. https://www.scienceopen.com/document?vid=28251d22-8476-40a6-916d-1a34796...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
