

Efficacy and safety of dupilumab for the treatment of uncontrolled asthma: a meta-analysis of randomized clinical trials
- PMID: 31151443
- PMCID: PMC6544936
- DOI: 10.1186/s12931-019-1065-3
Efficacy and safety of dupilumab for the treatment of uncontrolled asthma: a meta-analysis of randomized clinical trials
Abstract
Background: Several recent clinical trials have assessed the effects of dupilumab in uncontrolled asthma, but reached no definite conclusion. We therefore conducted this meta-analysis to evaluate the overall efficacy and safety of dupilumab for the treatment of uncontrolled asthma.
Methods: All randomized controlled trials were included. Standard mean differences (SMD) or relative risks (RR) were calculated using Fixed-or random-effects models.
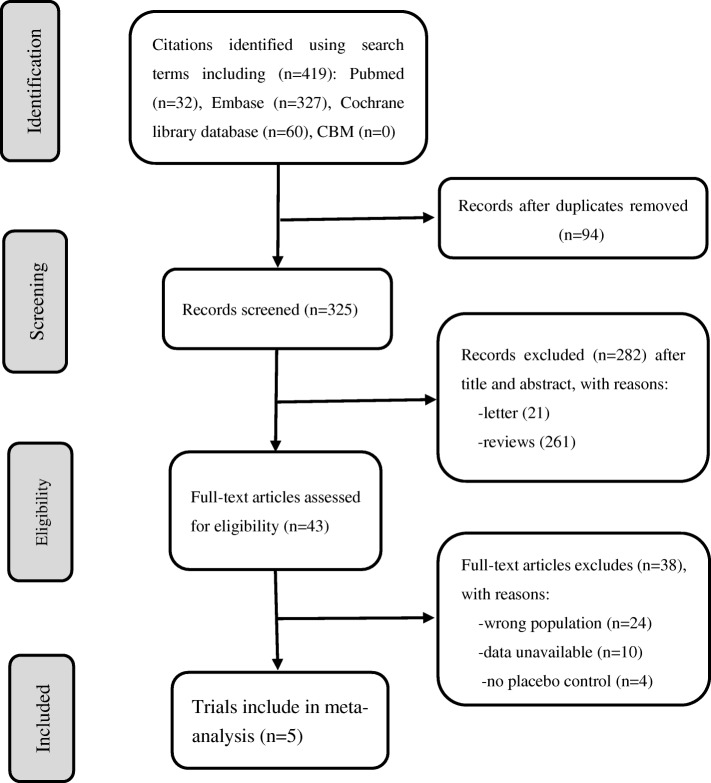
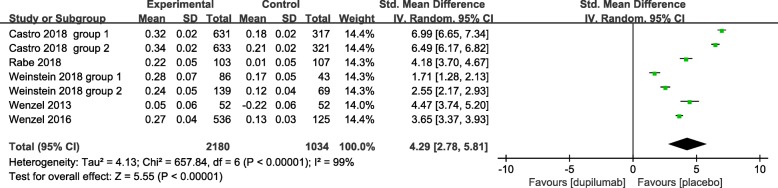
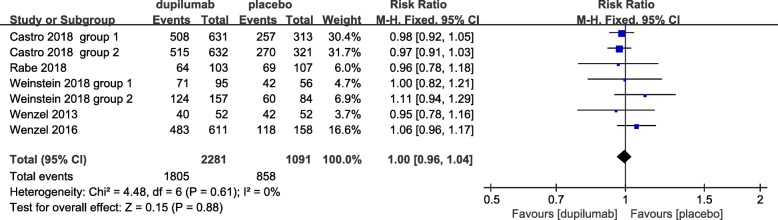
Results: Five studies involving 3369 patients were identified. Pooled analysis showed significant improvements in the first-second forced expiratory volume (FEV1) (SMD = 4.29, 95% CI: 2.78-5.81) and Asthma Quality of Life Questionnaire scores (SMD = 4.39, 95% CI: 1.44-7.34). Dupilumab treatments were also associated with significantly decreased 5-item Asthma Control Questionnaire scores (SMD = - 4.95, 95% CI: - 7.30 to - 2.60), AM and PM asthma symptom scores (SMD = - 5.09, 95% CI: - 6.40 to - 3.77; SMD = - 4.92, 95% CI: - 5.98 to - 3.86, respectively), and severe exacerbation risk (RR = 0.73; 95% CI: 0.67-0.79) compared with placebo, with similar incidence of adverse events (RR = 1.0; 95% CI: 0.96-1.04).
Conclusion: Dupilumab treatment is relatively well-tolerated and could significantly improve FEV1, symptoms, asthma control, and quality of life, and reduced severe exacerbation risk in patients with uncontrolled asthma.
Keywords: Dupilumab; Meta-analysis; Randomized control trial; Uncontrolled asthma.
Conflict of interest statement
The authors declare that they have no competing interest.
Figures








References
-
- Disease GBD, Injury I, Prevalence C. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the global burden of Disease study 2016. Lancet. 2017;390:1211–1259. doi: 10.1016/S0140-6736(17)32154-2. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
