

Combination of problem-based learning with high-fidelity simulation in CPR training improves short and long-term CPR skills: a randomised single blinded trial
- PMID: 31151450
- PMCID: PMC6544917
- DOI: 10.1186/s12909-019-1626-7
Combination of problem-based learning with high-fidelity simulation in CPR training improves short and long-term CPR skills: a randomised single blinded trial
Abstract
Background: Performance of sufficient cardiopulmonary resuscitation (CPR) by medical personnel is critical to improve outcomes during cardiac arrest. It has however been shown that even health care professionals possess a lack of knowledge and skills in CPR performance. The optimal method for teaching CPR remains unclear, and data that compares traditional CPR instructional methods with newer modalities of CPR instruction are needed. We therefore conducted a single blinded, randomised study involving medical students in order to evaluate the short- and long-term effects of a classical CPR education compared with a bilateral approach to CPR training, consisting of problem-based learning (PBL) plus high fidelity simulation.
Methods: One hundred twelve medical students were randomized during a curricular anaesthesiology course to a control (n = 54) and an intervention (n = 58) group. All participants were blinded to group assignment and partook in a 30-min-lecture on CPR basics. Subsequently, the control group participated in a 90-min tutor-guided CPR hands-on-training. The intervention group took part in a 45-min theoretical PBL module followed by 45 min of high fidelity simulated CPR training. The rate of participants recognizing clinical cardiac arrest followed by sufficiently performed CPR was the primary outcome parameter of this study. CPR performance was evaluated after the intervention. In addition, a follow-up evaluation was conducted after 6 months.
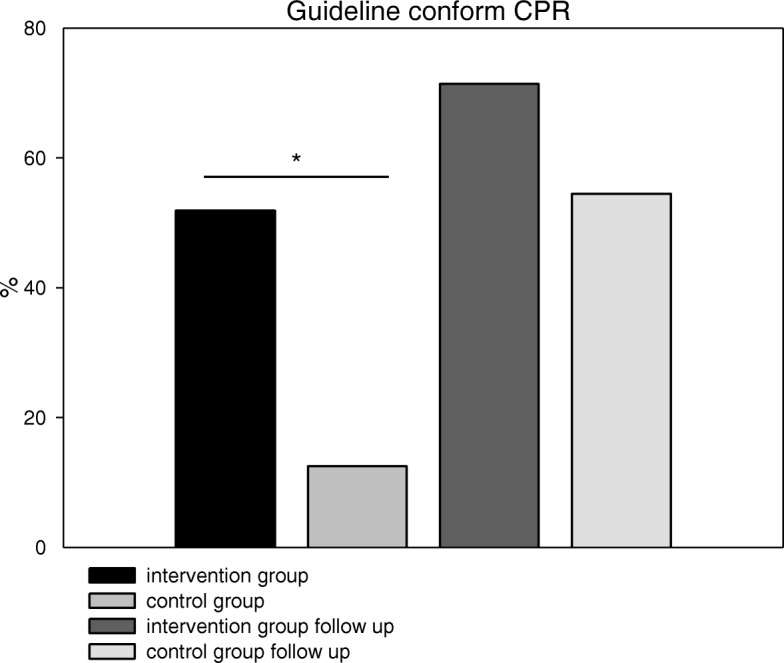
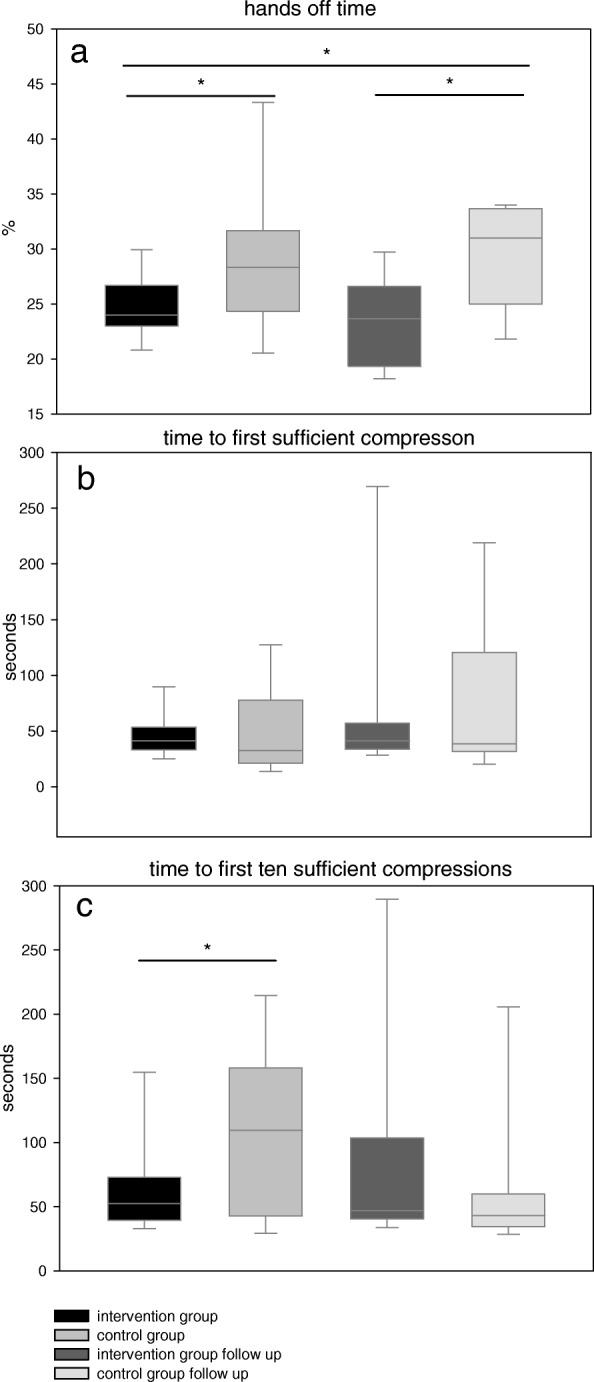
Results: 51.9% of the intervention group met the criteria of sufficiently performed CPR as compared to only 12.5% in the control group on the day of the intervention (p = 0.007). Hands-off-time as a marker for CPR continuity was significantly less in the intervention group (24.0%) as compared to the control group (28.3%, p = 0.007, Hedges' g = 1.55). At the six-month follow-up, hands-off-time was still significantly lower in the intervention group (23.7% vs. control group: 31.0%, p = 0.006, Hedges' g = 1.88) but no significant difference in sufficiently performed CPR was detected (intervention group: 71.4% vs. control group: 54.5%, p = 0.55).
Conclusion: PBL combined with high fidelity simulation training leads to a measurable short-term increase in initiating sufficient CPR by medical students immediately after training as compared to classical education. At six month post instruction, these differences remained only partially.
Keywords: Advanced adult CPR; Cardiopulmonary resuscitation; Hands-on training; High-fidelity simulation; Medical students’ education; Problem-based learning.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Healey A, Sherbino J, Fan J, Mensour M, Upadhye S, Wasi P. A low-fidelity simulation curriculum addresses needs identified by faculty and improves the comfort level of senior internal medicine resident physicians with inhospital resuscitation. Crit Care Med. 2010;38:1899–1903. doi: 10.1097/CCM.0b013e3181eb3ca9. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
