

Sociodemographic variation in the oral microbiome
- PMID: 31151886
- PMCID: PMC6626698
- DOI: 10.1016/j.annepidem.2019.03.006
Sociodemographic variation in the oral microbiome
Abstract
Purpose: Variations in the oral microbiome are potentially implicated in social inequalities in oral disease, cancers, and metabolic disease. We describe sociodemographic variation of oral microbiomes in a diverse sample.
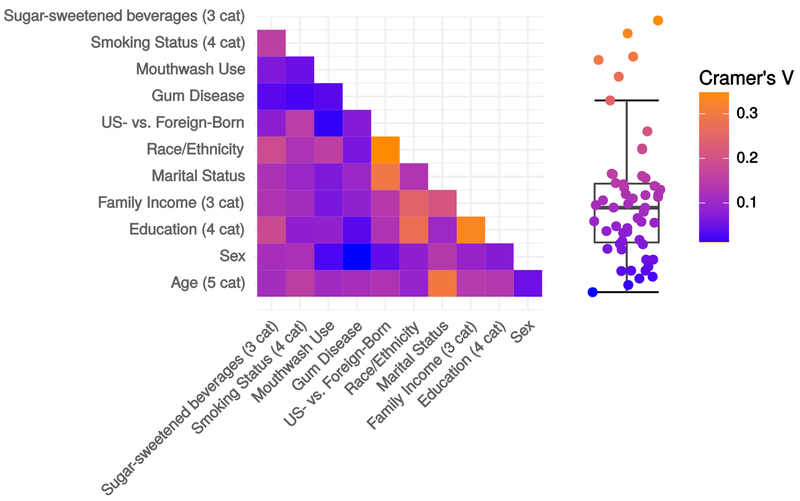
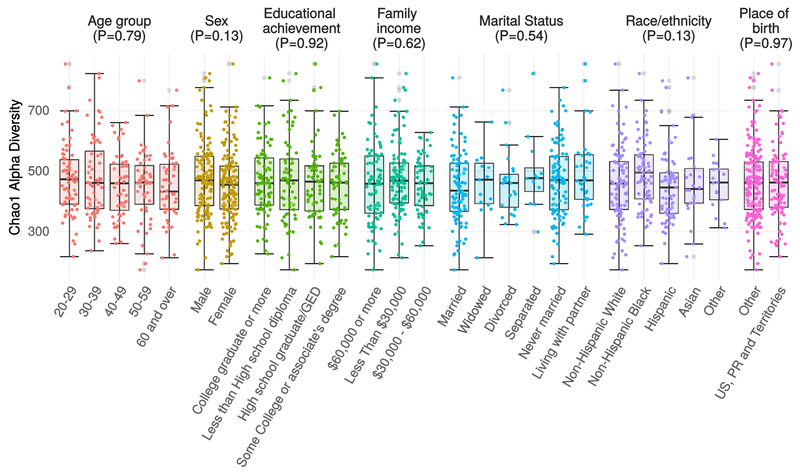
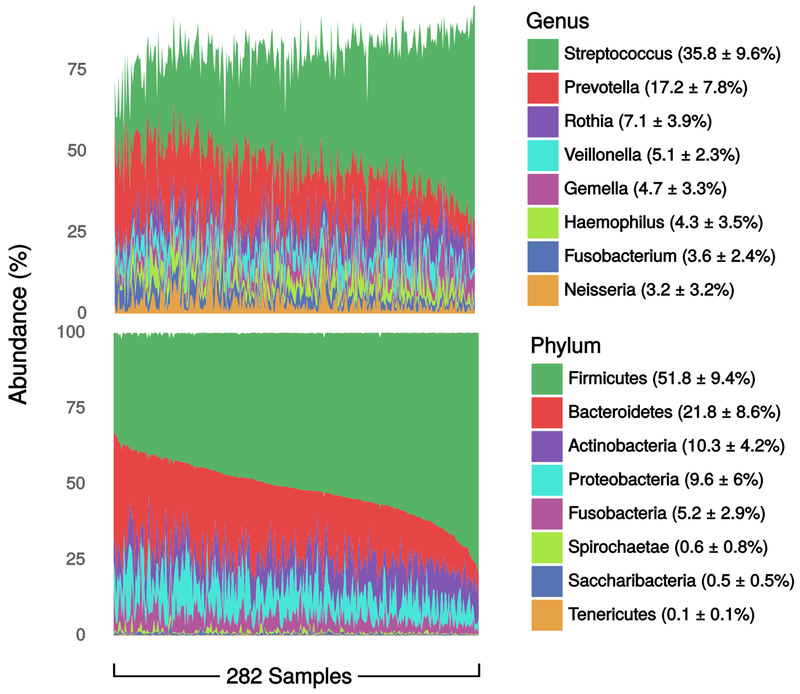
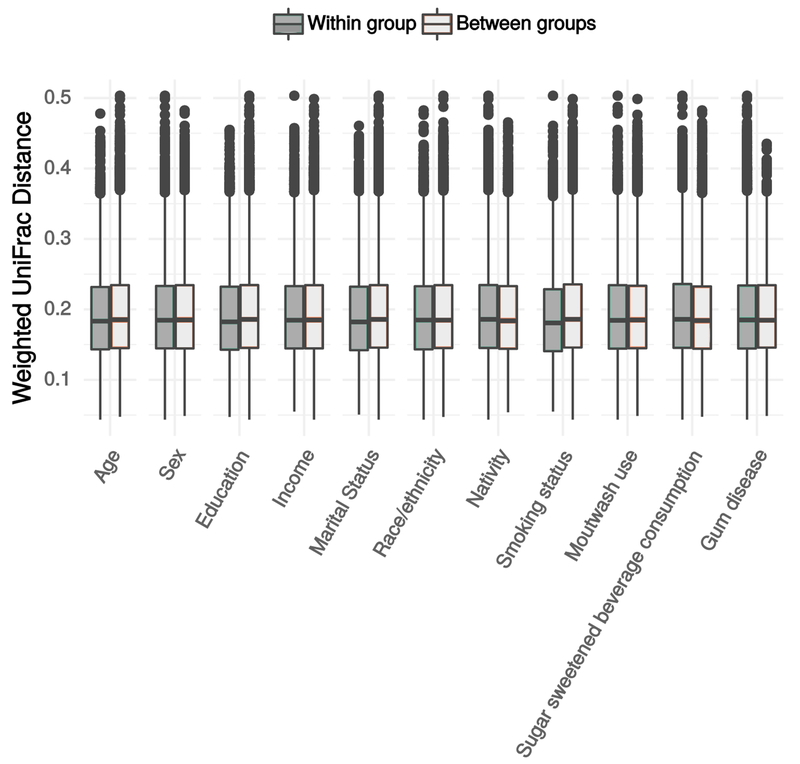
Methods: We performed 16S rRNA sequencing on mouthwash specimens in a subsample (n = 282) of the 2013-2014 population-based New York City Health and Nutrition Examination Study. We examined differential abundance of 216 operational taxonomic units, and alpha and beta diversity by age, sex, income, education, nativity, and race/ethnicity. For comparison, we examined differential abundance by diet, smoking status, and oral health behaviors.
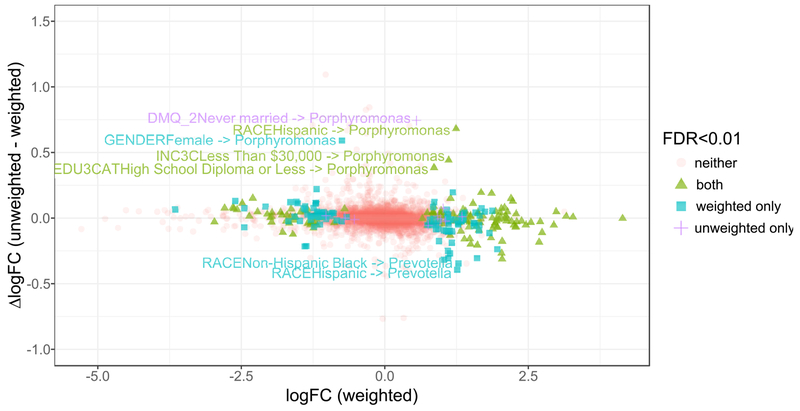
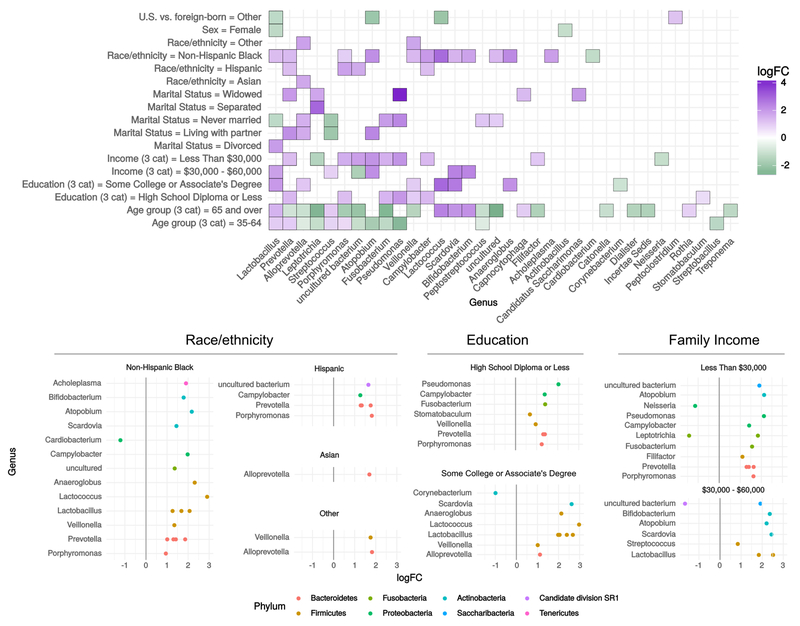
Results: Sixty-nine operational taxonomic units were differentially abundant by any sociodemographic variable (false discovery rate < 0.01), including 27 by race/ethnicity, 21 by family income, 19 by education, 3 by sex. We found 49 differentially abundant by smoking status, 23 by diet, 12 by oral health behaviors. Genera differing for multiple sociodemographic characteristics included Lactobacillus, Prevotella, Porphyromonas, Fusobacterium.
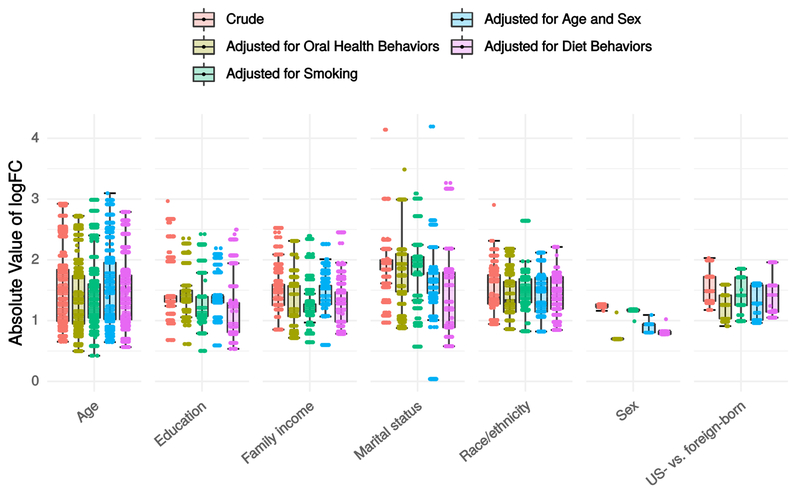
Conclusions: We identified oral microbiome variation consistent with health inequalities, more taxa differing by race/ethnicity than diet, and more by SES variables than oral health behaviors. Investigation is warranted into possible mediating effects of the oral microbiome in social disparities in oral and metabolic diseases and cancers.
Keywords: Demographics; Health disparities; Oral microbiome; Social epidemiology.
Copyright © 2019 Elsevier Inc. All rights reserved.
Figures
References
-
- Beckles GL, Chou C-F. Disparities in the Prevalence of Diagnosed Diabetes - United States, 1999-2002 and 2011-2014. MMWR Morb Mortal Wkly Rep 2016;65(45):1265–9. - PubMed
-
- Aiello AE, Dowd JB. Socio-economic Status and Immunosenescence Immunosenescence: Springer, New York, NY; 2013. p. 145–57.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
