

Scale-up of radiotherapy for cervical cancer in the era of human papillomavirus vaccination in low-income and middle-income countries: a model-based analysis of need and economic impact
- PMID: 31151906
- PMCID: PMC7055962
- DOI: 10.1016/S1470-2045(19)30308-0
Scale-up of radiotherapy for cervical cancer in the era of human papillomavirus vaccination in low-income and middle-income countries: a model-based analysis of need and economic impact
Abstract
Background: Radiotherapy is standard of care for cervical cancer, but major global gaps in access exist, particularly in low-income and middle-income countries. We modelled the health and economic benefits of a 20-year radiotherapy scale-up to estimate the long-term demand for treatment in the context of human papillomavirus (HPV) vaccination.
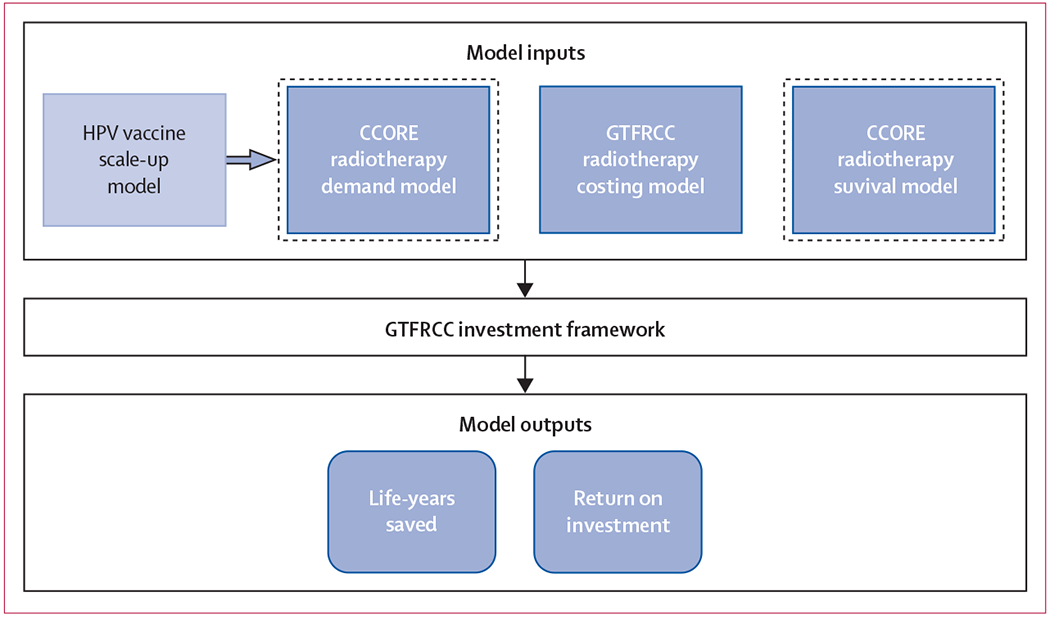
Methods: We applied the Global Task Force on Radiotherapy for Cancer Control investment framework to model the health and economic benefits of scaling up external-beam radiotherapy and brachytherapy for cervical cancer in upper-middle-income, lower-middle-income, and low-income countries between 2015 and 2035. We estimated the unique costs of external-beam radiotherapy and brachytherapy and included a specific valuation of women's caregiving contributions. Model outcomes life-years gained and the human capital and full income net present value of investment. We estimated the effects of stage at diagnosis, radiotherapy delivery system, and simultaneous HPV vaccination (75% coverage) up to a time horizon set at 2072.
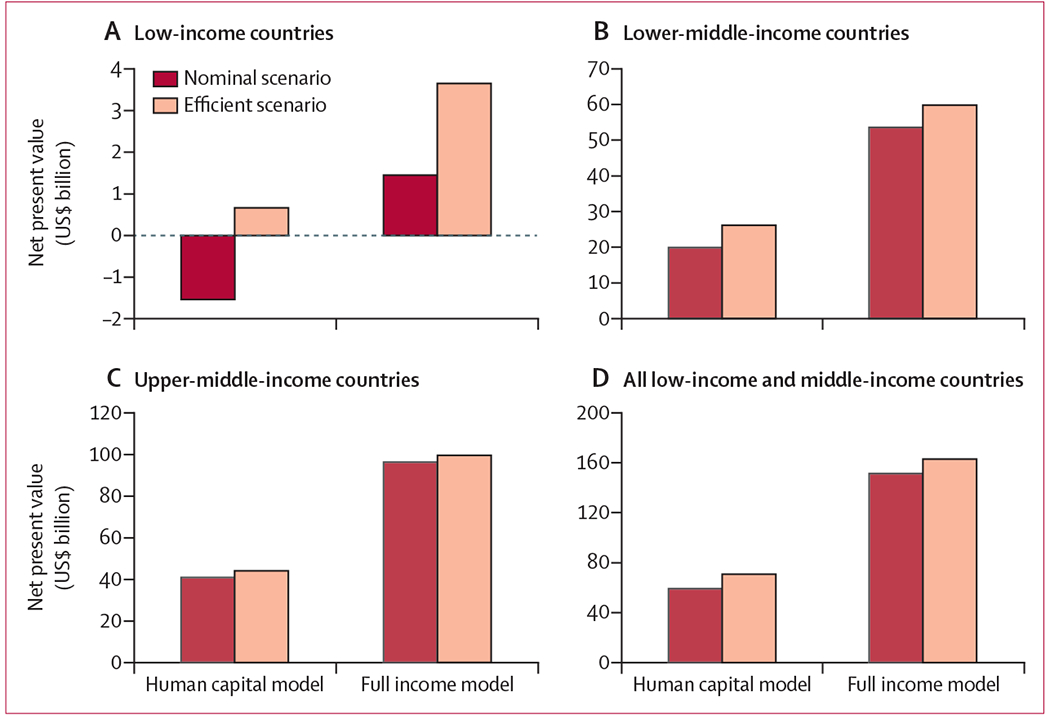
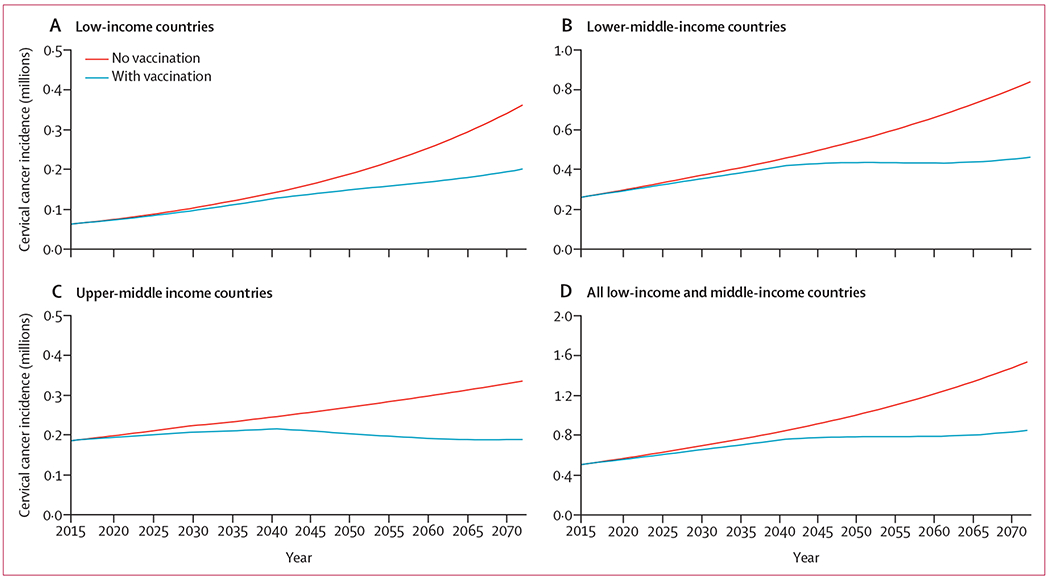
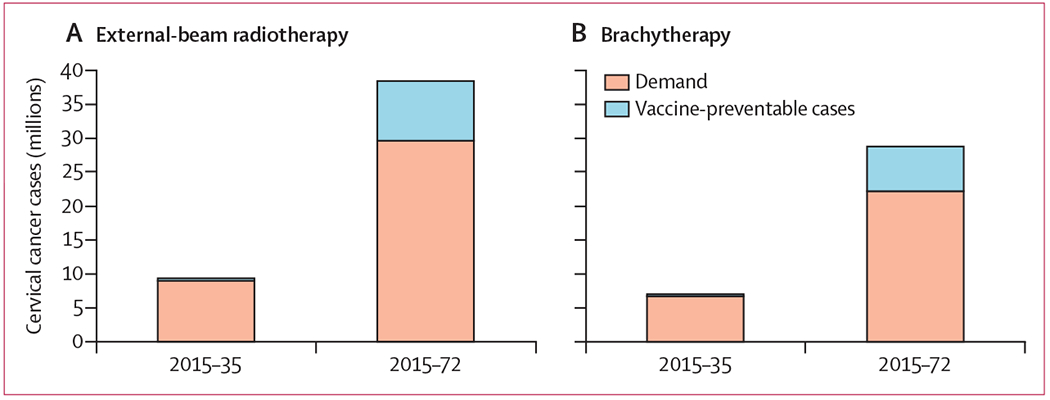
Findings: For the period from 2015 to 2035, we estimated that 9·4 million women in low-income and middle-income countries required treatment with external-beam radiotherapy, of which 7·0 million also required treatment with brachytherapy. Incremental scale-up of radiotherapy in these countries from 2015 to meet optimal radiotherapy demand by 2035 yielded 11·4 million life-years gained, $59·3 billion in human capital net present value (-$1·5 billion in low-income, $19·9 billion in lower-middle-income, and $40·9 billion in upper-middle-income countries), and $151·5 billion in full income net present value ($1·5 billion in low-income countries, $53·6 billion in lower-middle-income countries, and $96·4 billion in upper-middle-income countries). Benefits increased with advanced stage of cervical cancer and more efficient scale up of radiotherapy. Bivalent HPV vaccination of 12-year-old girls resulted in a 3·9% reduction in incident cases from 2015-2035. By 2072, when the first vaccinated cohort of girls reaches 70 years of age, vaccination yielded a 22·9% reduction in cervical cancer incidence, with 38·4 million requiring external-beam radiotherapy and 28·8 million requiring brachytherapy.
Interpretation: Effective cervical cancer control requires a comprehensive strategy. Even with HPV vaccination, radiotherapy treatment scale-up remains essential and produces large health benefits and a strong return on investment to countries at different levels of development.
Funding: None.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests
We declare no competing interests.
Figures
Comment in
-
Scale-up of radiotherapy for cervical cancer.Lancet Oncol. 2019 Jul;20(7):888-889. doi: 10.1016/S1470-2045(19)30376-6. Epub 2019 May 28. Lancet Oncol. 2019. PMID: 31151903 No abstract available.
References
-
- Ferlay J, Colombet M, Soerjomataram I, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer 2018; 144: 1941–53. - PubMed
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68: 394–424. - PubMed
-
- Knaul FM, Farmer PE, Krakauer EL, et al. Alleviating the access abyss in palliative care and pain relief-an imperative of universal health coverage: the Lancet Commission report. Lancet 2018; 391: 1391–454. - PubMed
-
- Atun R, Jaffray DA, Barton MB, et al. Expanding global access to radiotherapy. Lancet Oncol 2015; 16: 1153–86. - PubMed
-
- Rodin D, Grover S, Elmore SN, et al. The power of integration: radiotherapy and global palliative care. Ann Palliat Med 2016; 5: 209–17 - PubMed
