

Intrathecal administration of autologous mesenchymal stem cells in multiple system atrophy
- PMID: 31152011
- PMCID: PMC6659003
- DOI: 10.1212/WNL.0000000000007720
Intrathecal administration of autologous mesenchymal stem cells in multiple system atrophy
Abstract
Objective: This phase I/II study sought to explore intrathecal administration of mesenchymal stem cells (MSCs) as therapeutic approach to multiple system atrophy (MSA).
Methods: Utilizing a dose-escalation design, we delivered between 10 and 200 million adipose-derived autologous MSCs intrathecally to patients with early MSA. Patients were closely followed with clinical, laboratory, and imaging surveillance. Primary endpoints were frequency and type of adverse events; key secondary endpoint was the rate of disease progression assessed by the Unified MSA Rating Scale (UMSARS).
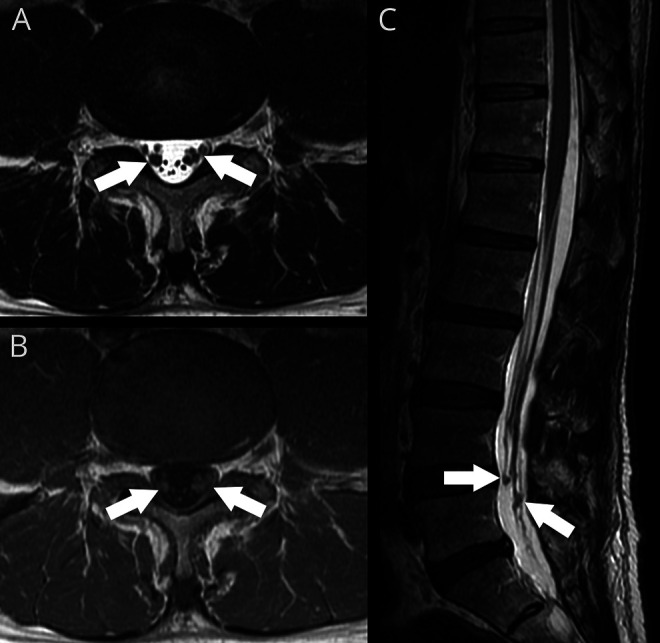
Results: Twenty-four patients received treatment. There were no attributable serious adverse events, and injections were generally well-tolerated. At the highest dose tier, 3 of 4 patients developed low back/posterior leg pain, associated with thickening/enhancement of lumbar nerve roots. Although there were no associated neurologic deficits, we decided that dose-limiting toxicity was reached. A total of 6 of 12 patients in the medium dose tier developed similar, but milder and transient discomfort. Rate of progression (UMSARS total) was markedly lower compared to a matched historical control group (0.40 ± 0.59 vs 1.44 ± 1.42 points/month, p = 0.004) with an apparent dose-dependent effect.
Conclusions: Intrathecal MSC administration in MSA is safe and well-tolerated but can be associated with a painful implantation response at high doses. Compelling dose-dependent efficacy signals are the basis for a planned placebo-controlled trial.
Classification of evidence: This phase I/II study provides Class IV evidence that for patients with early MSA, intrathecal MSC administration is safe, may result in a painful implantation response at high doses, and is associated with dose-dependent efficacy signals.
© 2019 American Academy of Neurology.
Figures




Comment in
-
Comment: Autologous mesenchymal stem cells: Hope for patients with multiple system atrophy?Neurology. 2019 Jul 2;93(1):25. doi: 10.1212/WNL.0000000000007721. Epub 2019 May 31. Neurology. 2019. PMID: 31152012 No abstract available.
References
-
- Gilman S, Low PA, Quinn N, et al. . Consensus statement on the diagnosis of multiple system atrophy. J Auton Nerv Syst 1998;74:189–192. - PubMed
-
- Benarroch EE, Schmeichel AM, Parisi JE. Depletion of mesopontine cholinergic and sparing of raphe neurons in multiple system atrophy. Neurology 2002;59:944–946. - PubMed
-
- Wakabayashi K, Takahashi H. Cellular pathology in multiple system atrophy. Neuropathology 2006;26:338–345. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials