

Different microvascular alterations underlie microbleeds and microinfarcts
- PMID: 31152566
- PMCID: PMC8722100
- DOI: 10.1002/ana.25512
Different microvascular alterations underlie microbleeds and microinfarcts
Abstract
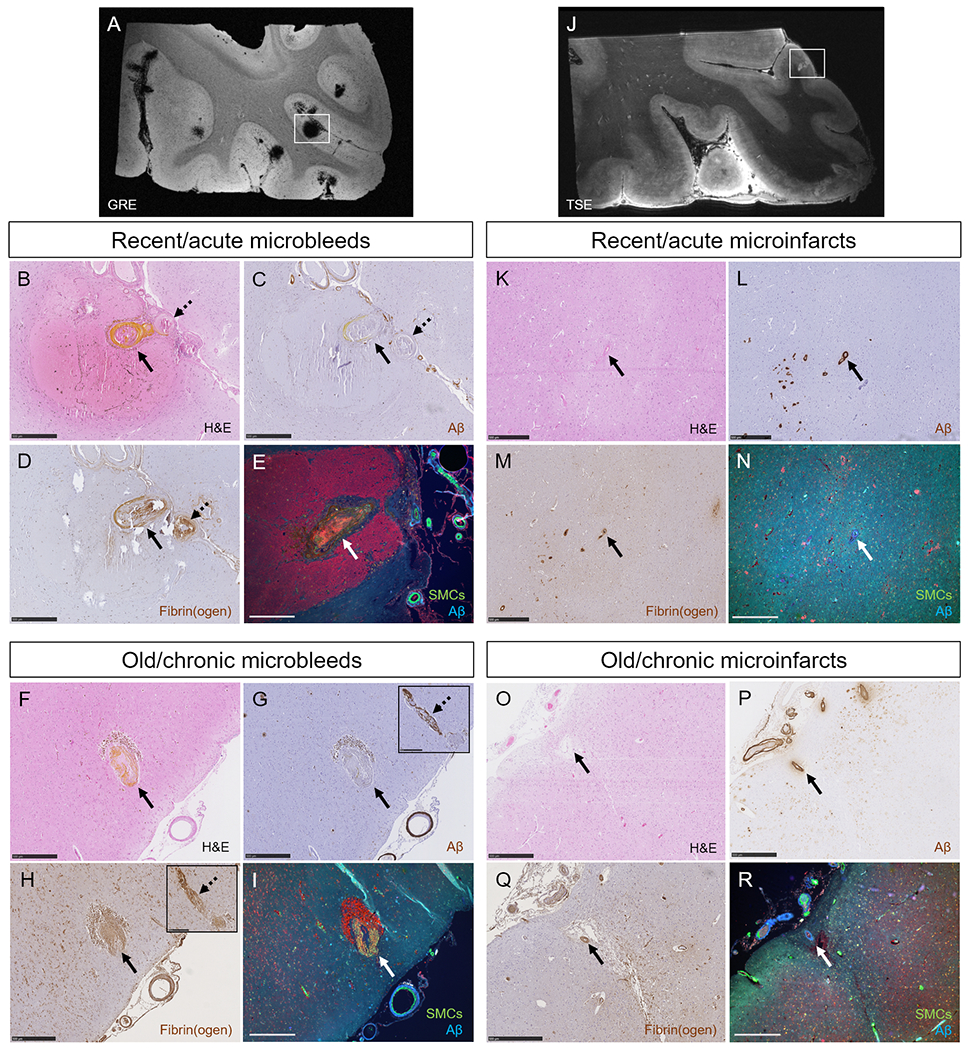
Objective: Cerebral amyloid angiopathy (CAA) is characterized by the accumulation of amyloid β (Aβ) in the walls of cortical vessels and the accrual of microbleeds and microinfarcts over time. The relationship between CAA severity and microbleeds and microinfarcts as well as the sequence of events that lead to lesion formation remain poorly understood.
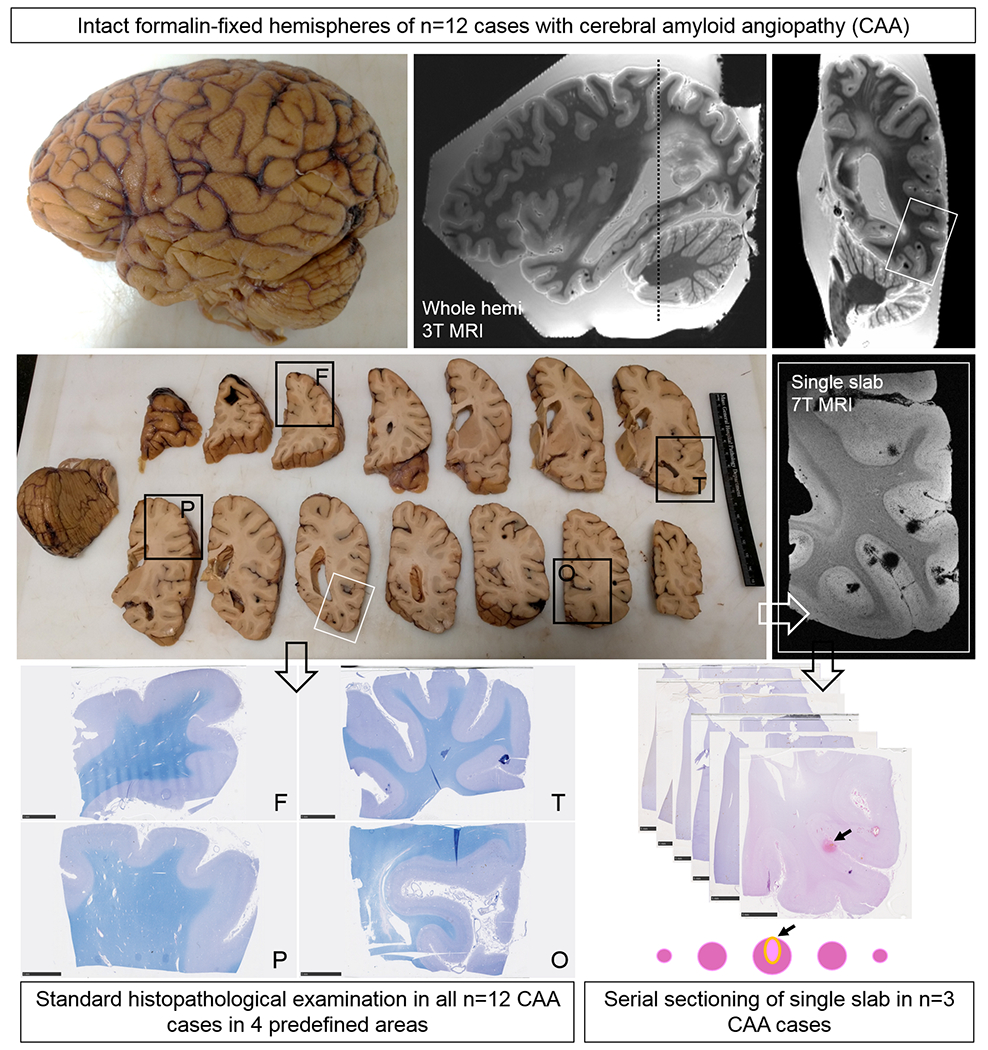
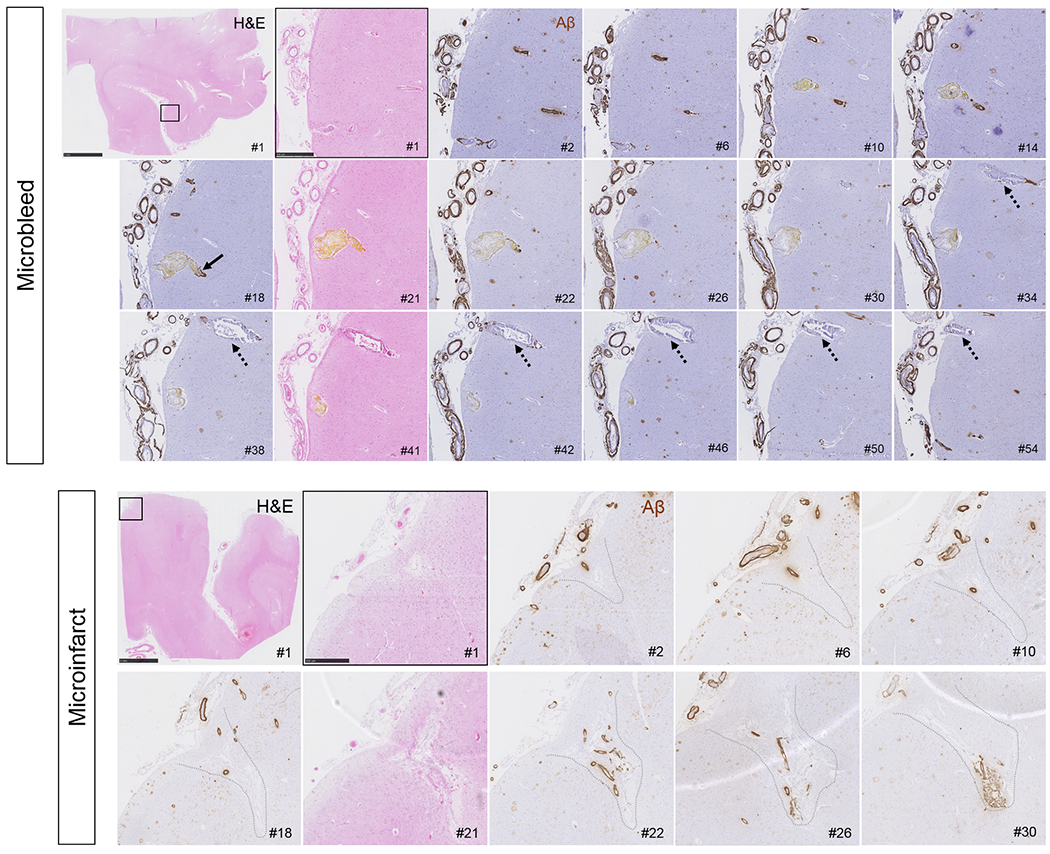
Methods: We scanned intact formalin-fixed hemispheres of 12 CAA cases with magnetic resonance imaging (MRI), followed by histopathological examination in predefined areas and serial sectioning in targeted areas with multiple lesions.
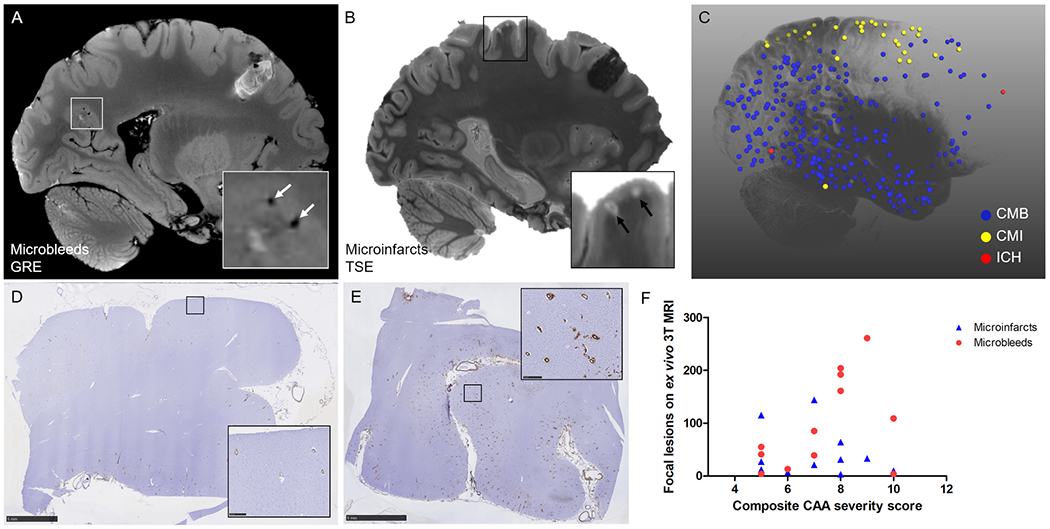
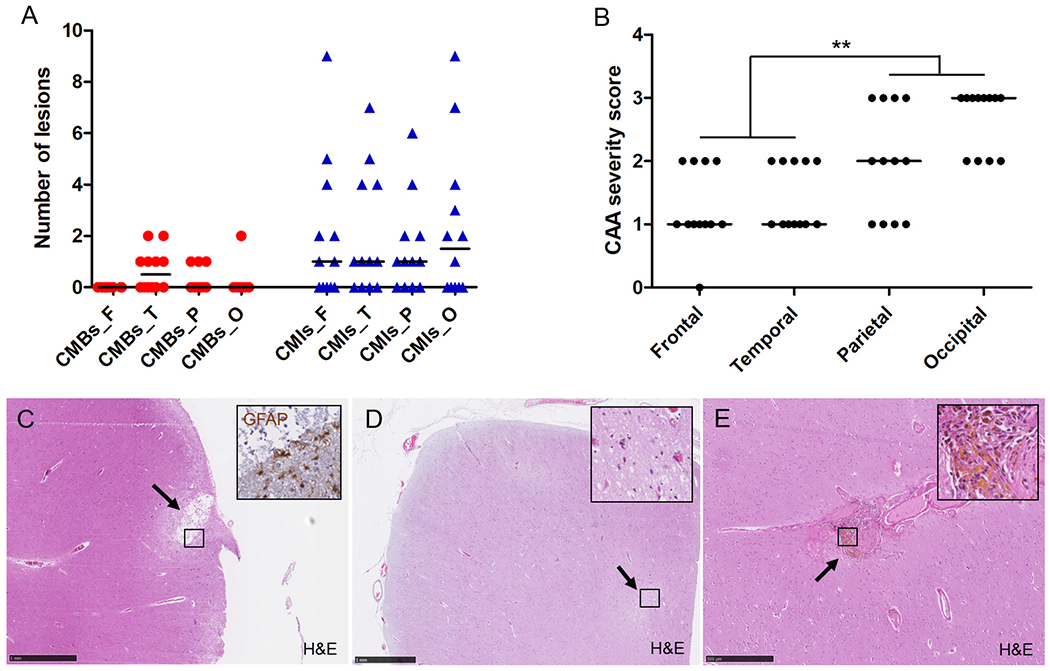
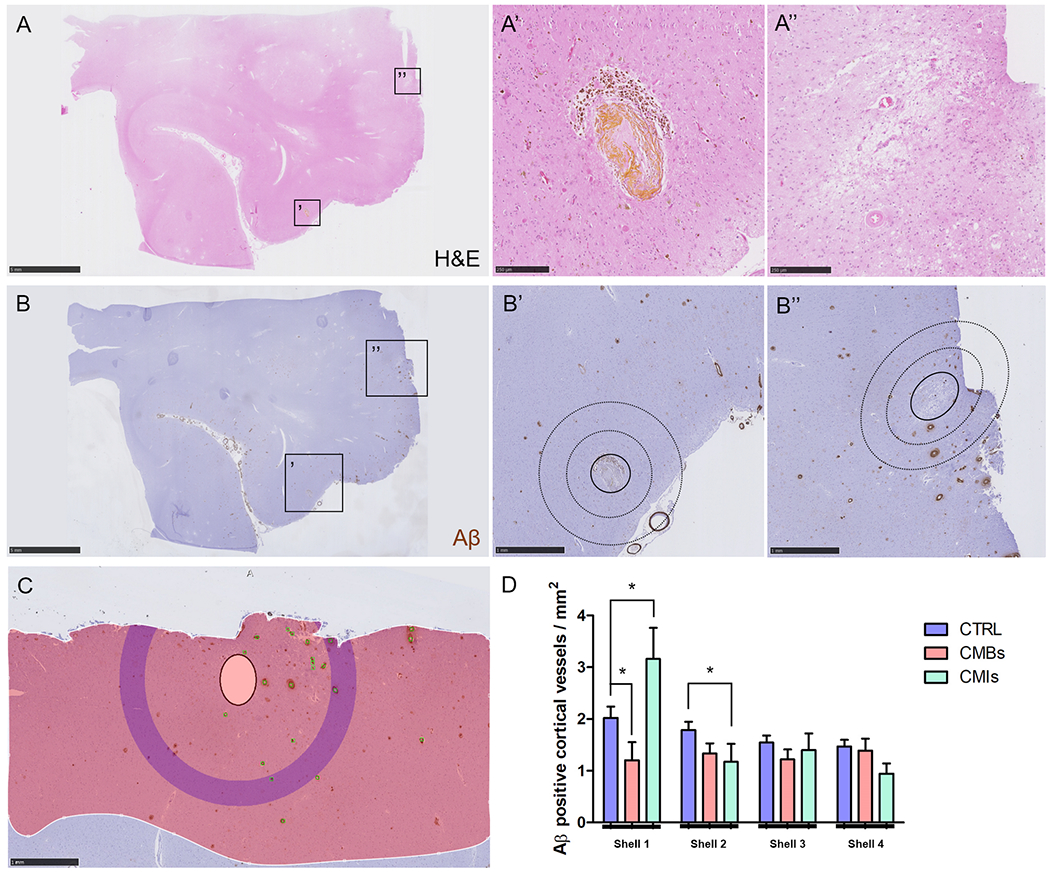
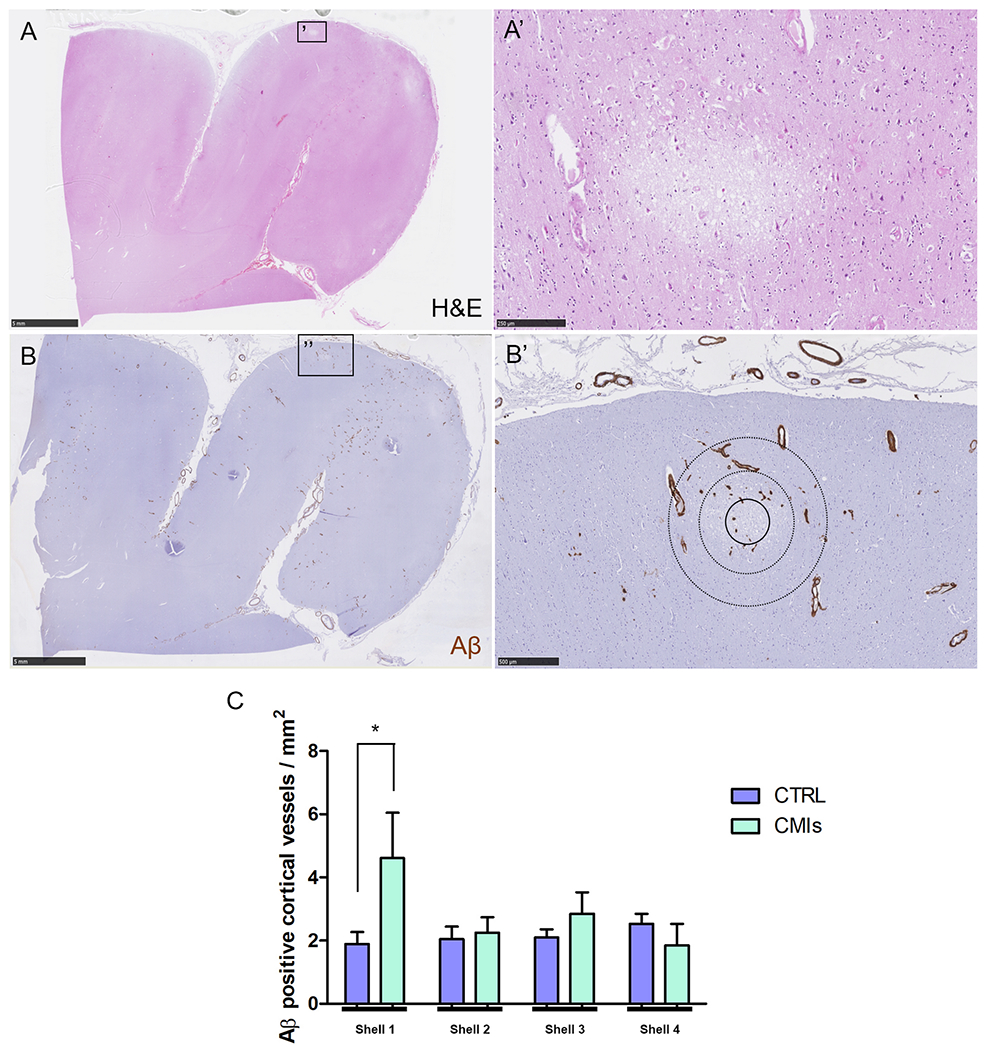
Results: In total, 1,168 cortical microbleeds and 472 cortical microinfarcts were observed on ex vivo MRI. Increasing CAA severity at the whole-brain or regional level was not associated with the number of microbleeds or microinfarcts. However, locally, the density of Aβ-positive cortical vessels was lower surrounding a microbleed compared to a simulated control lesion, and higher surrounding microinfarcts. Serial sectioning revealed that for (n = 28) microbleeds, both Aβ (4%) and smooth muscle cells (4%) were almost never present in the vessel wall at the site of bleeding, but Aβ was frequently observed upstream or downstream (71%), as was extensive fibrin(ogen) buildup (87%). In contrast, for (n = 22) microinfarcts, vascular Aβ was almost always observed at the core of the lesion (91%, p < 0.001) as well as upstream or downstream (82%), but few vessels associated with microinfarcts had intact smooth muscle cells (9%).
Interpretation: These observations provide a model for how a single neuropathologic process such as CAA may result in hemorrhagic or ischemic brain lesions potentially through 2 different mechanistic pathways. ANN NEUROL 2019;86:279-292.
© 2019 American Neurological Association.
Conflict of interest statement
Potential conflicts of interest
Nothing to report.
Figures
References
Publication types
MeSH terms
Grants and funding
- K99 AG059893/AG/NIA NIH HHS/United States
- RF1 NS110054/NH/NIH HHS/United States
- R21 AG046657/NH/NIH HHS/United States
- P30 AG062421/AG/NIA NIH HHS/United States
- K99 AG059893/NH/NIH HHS/United States
- 91619021/Nederlandse Organisatie voor Wetenschappelijk Onderzoek/International
- 019.153LW.014/Nederlandse Organisatie voor Wetenschappelijk Onderzoek/International
- R01 NS096730/NS/NINDS NIH HHS/United States
- RF1 NS110054/NS/NINDS NIH HHS/United States
- R21 AG046657/AG/NIA NIH HHS/United States
- R01 NS096730/NH/NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
