

Functional fibrinogen (FLEV-TEG) versus the Clauss method in an obstetric population: a comparative study
- PMID: 31153366
- PMCID: PMC6545203
- DOI: 10.1186/s12871-019-0769-8
Functional fibrinogen (FLEV-TEG) versus the Clauss method in an obstetric population: a comparative study
Abstract
Background: Hemostasis is the dynamic equilibrium between coagulation and fibrinolysis. During pregnancy, the balance shifts toward a hypercoagulative state; however placental abruption and abnormal placentations may lead to rapidly evolving coagulopathy characterized by the increased activation of procoagulant pathways. These processes can result in hypofibrinogenemia, with fibrinogen levels dropping to 2 g/L or less and an associated increased risk of post-partum hemorrhage. The aim of the present study was to evaluate the concordance between two methods of functional fibrinogen measurement: the Thromboelastography (TEG) method (also known as FLEV) vs. the Clauss method. Three patient groups were considered: healthy volunteers; non-pathological pregnant patients; and pregnant patients who went on to develop postpartum hemorrhage.
Methods: A prospective observational study. Inclusion criteria were: healthy volunteer women of childbearing age, non-pathological pregnant women at term, and pregnant hemorrhagic patients subjected to elective or urgent caesarean section (CS), with blood loss exceeding 1000 mL. Exclusion criteria were age < 18 years, a history of coagulopathy, and treatment with contraceptives, anticoagulants, or antiplatelet agents.
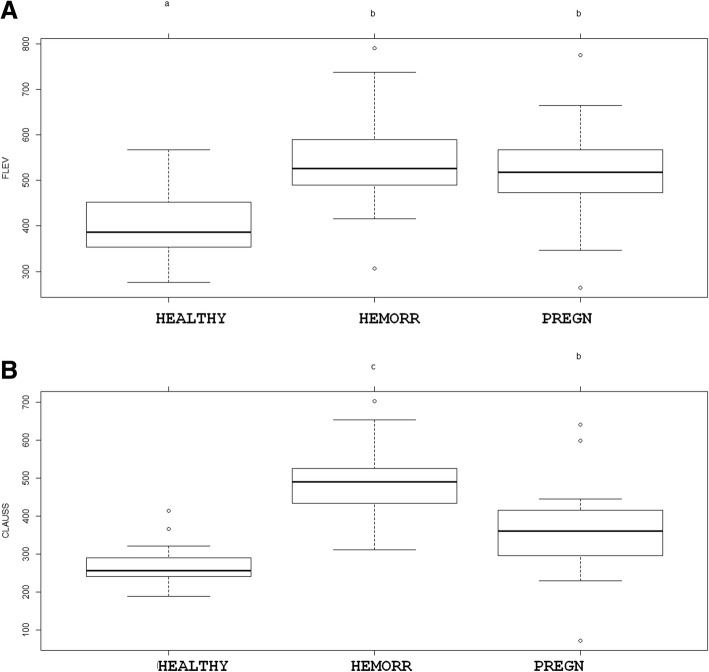
Results: Bland-Altman plots showed a significant overestimation with the FLEV method in all three patient groups: bias was - 133.36 mg/dL for healthy volunteers (95% IC: - 257.84; - 8.88. Critical difference: 124.48); - 56.30 mg/dL for healthy pregnant patients (95% IC: - 225.53; 112.93. Critical difference: 169.23); and - 159.05 mg/dL for hemorrhagic pregnant patients (95% IC: - 333.24; 15.148. Critical difference: 174.19). Regression analyses detected a linear correlation between FLEV and Clauss for healthy volunteers, healthy pregnant patients, and hemorrhagic pregnant patients (R2 0.27, p value = 0.002; R2 0.31, p value = 0.001; R2 0.35, p value = 0.001, respectively). ANOVA revealed a statistically significant difference in fibrinogen concentration between all three patients groups when assayed using the Clauss method (p value < 0.001 for all the comparisons), but no statistically significant difference between the two patients groups of pregnant women when using the FLEV method.
Conclusions: The FLEV method does not provide a valid alternative to the Clauss method due to the problem of fibrinogen overestimation, and for this reason it should not be recommended for the evaluation of patients with an increased risk of hypofibrinogenemia.
Keywords: Coagulopathy; Fibrinogen; Post-partum hemorrhage; Thromboelastography.
Conflict of interest statement
Dr. Luigi Vetrugno is Associate Editor of BMC Anesthesiology. No competing interests for the other Authors.
Figures

References
-
- Bremme K, Ostlund E, Almqvist I, Heinonen K, Blombäck M. Enhanced thrombin generation and fibrinolytic activity in normal pregnancy and the puerperium. Obstet Gynecol. 1992;80:132–137. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
