

Accuracy of MRI in diagnosing intra-articular pathology of the long head of the biceps tendon: results with a large cohort of patients
- PMID: 31153372
- PMCID: PMC6545217
- DOI: 10.1186/s12891-019-2654-5
Accuracy of MRI in diagnosing intra-articular pathology of the long head of the biceps tendon: results with a large cohort of patients
Abstract
Background: It is difficult to diagnose the pathology of the long head of the biceps tendon (LHBT) clinically. This study aimed to determine the diagnostic value of standard non-enhancing magnetic resonance imaging (MRI) for detecting LHBT pathology and identify the most useful diagnostic signs on MRI.
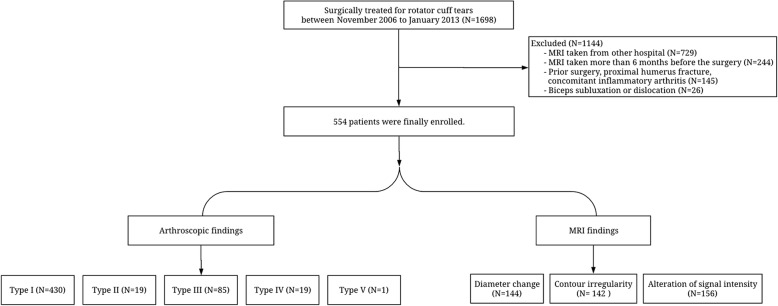
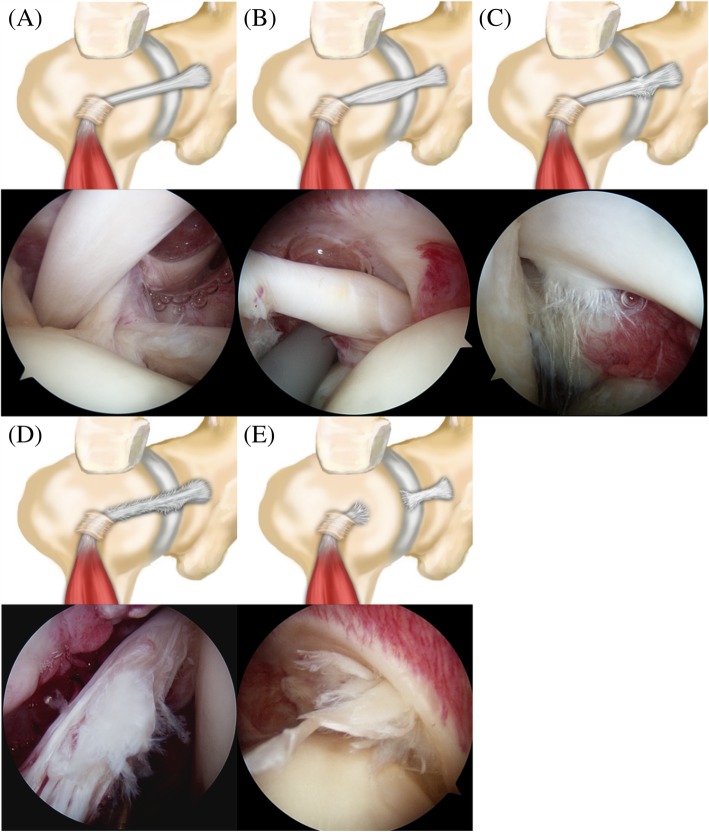
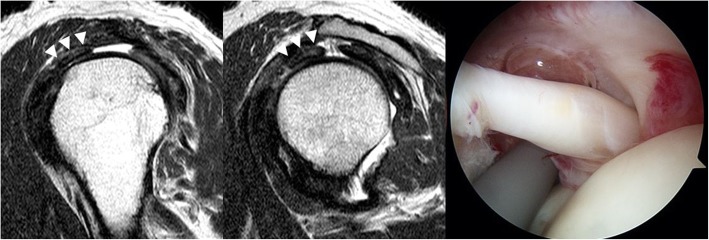
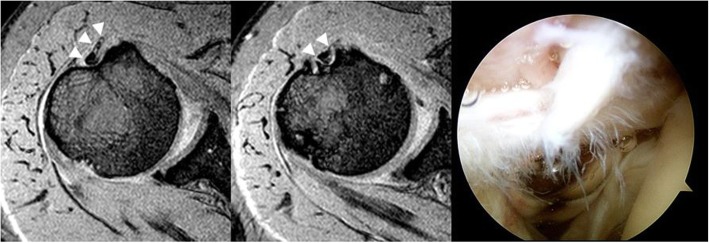
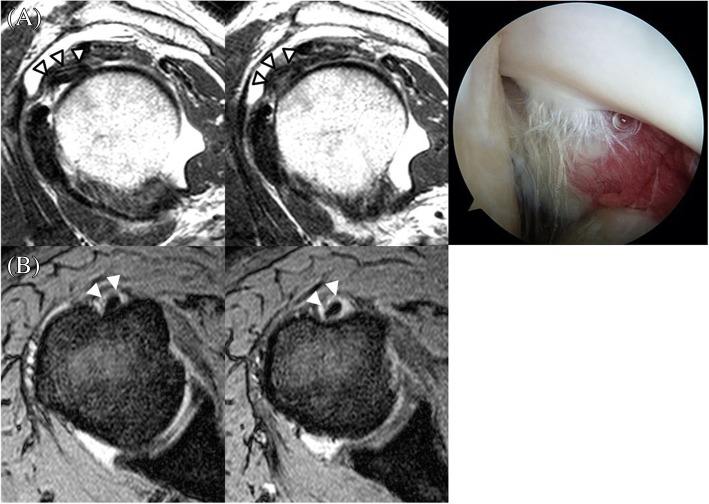
Methods: A total of 554 patients with preoperative 3-Tesla (3 T) MRI who underwent arthroscopic surgery for rotator cuff tears were retrospectively enrolled. Abnormal signs of LHBT on MRI included diameter change, contour irregularity, and alteration of signal intensity. Arthroscopic findings were classified according to tear progress and used as a reference standard: Type I, normal tendon; Type II, hourglass-shaped hypertrophic tendon with fraying extending into the bicipital groove; Type III, partial tear involving less than 50% of tendon width at the intraarticular region without fraying in the bicipital groove; Type IV, partial tear involving more than 50% of tendon width and extending into the bicipital groove; and Type V, complete tear (cutoff) of the tendon. Using receiver operating characteristic, prediction accuracies of MRI findings were assessed compared to those of arthroscopic findings.
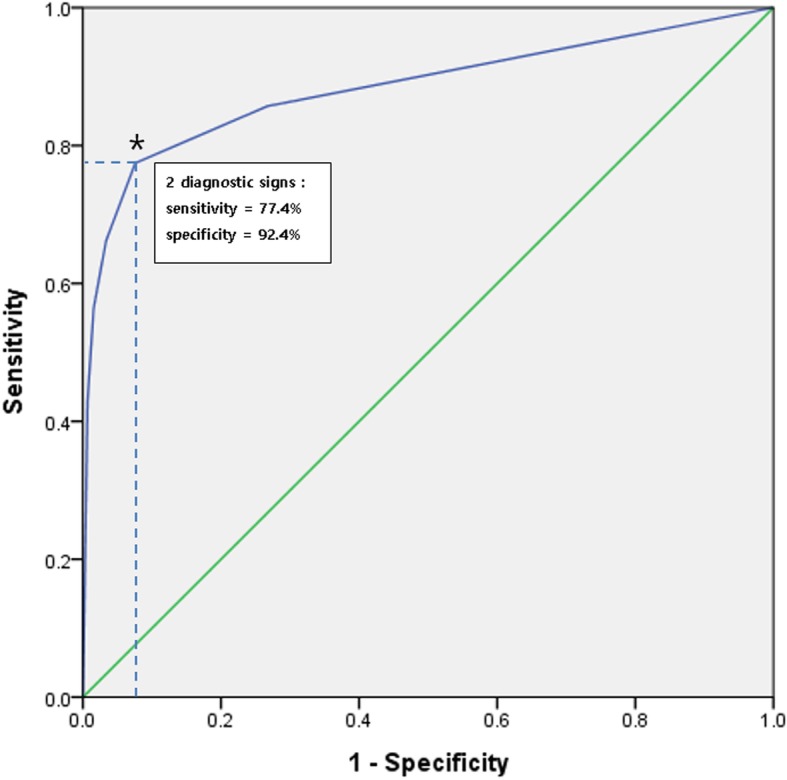
Results: Arthroscopic findings showed LHBT pathology in 124 (22.4%) cases. High diagnostic efficacy was achieved when 'at least 2 abnormal signs' was set as diagnostic criteria (sensitivity: 77.9%; specificity: 93.7%; positive predictive value: 76.3%). Types II and III lesions showed the highest sensitivities (36.8 and 66.7%, respectively) in abnormal alteration of signal intensity in the parasagittal view while Type IV showed the highest sensitivity (82.3%) in diameter change in axial view. Interobserver agreements were substantial to almost perfect, with kappa value of 0.69-0.81.
Conclusions: The standard non-enhancing 3 T MRI had a high diagnostic value in preoperative detection of LHBT pathology. Its accuracy was increased when diagnostic criterion was set as '2 or more abnormal signs (diameter change, contour irregularity, and alteration of signal intensity)'. The single diagnostic sign with the highest sensitivity was alteration of signal intensity in the parasagittal view.
Keywords: Diagnostic criteria; Diagnostic efficacy; Long head of biceps tendon; Magnetic resonance imaging; Shoulder.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Barber FA, Field LD, Ryu RK. Biceps tendon and superior labrum injuries: decision making. Instr Course Lect. 2008;57:527–538. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
