

Temporal Trends in the Use of Acute Recanalization Therapies for Ischemic Stroke in Patients with Cancer
- PMID: 31153762
- PMCID: PMC6679738
- DOI: 10.1016/j.jstrokecerebrovasdis.2019.05.009
Temporal Trends in the Use of Acute Recanalization Therapies for Ischemic Stroke in Patients with Cancer
Abstract
Objective: We sought to characterize the US nationwide temporal trends in recanalization therapy utilization for ischemic stroke among patients with and without cancer.
Methods: We identified all acute ischemic stroke (AIS) hospitalizations in the National Inpatient Sample from January 1, 1998 to September 30, 2015. The primary exposure was solid or hematologic cancer. The primary outcome was use of intravenous thrombolysis. The secondary outcome was use of endovascular therapy (EVT).
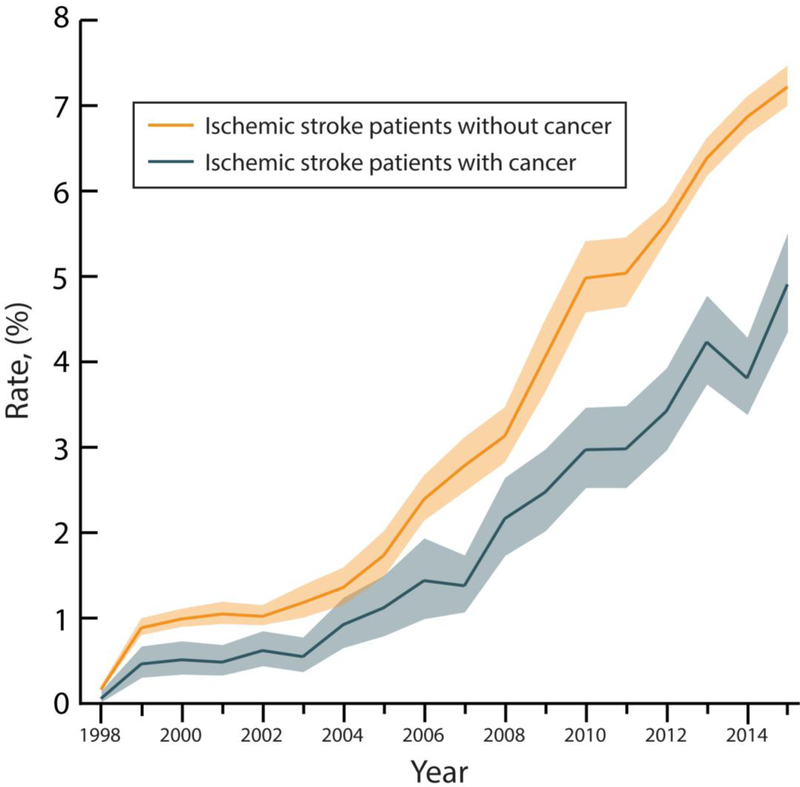
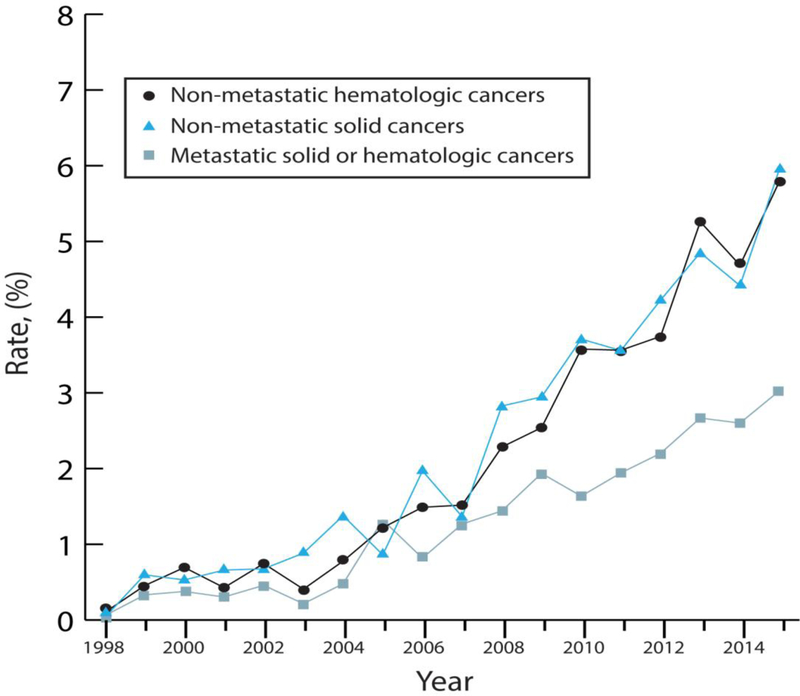
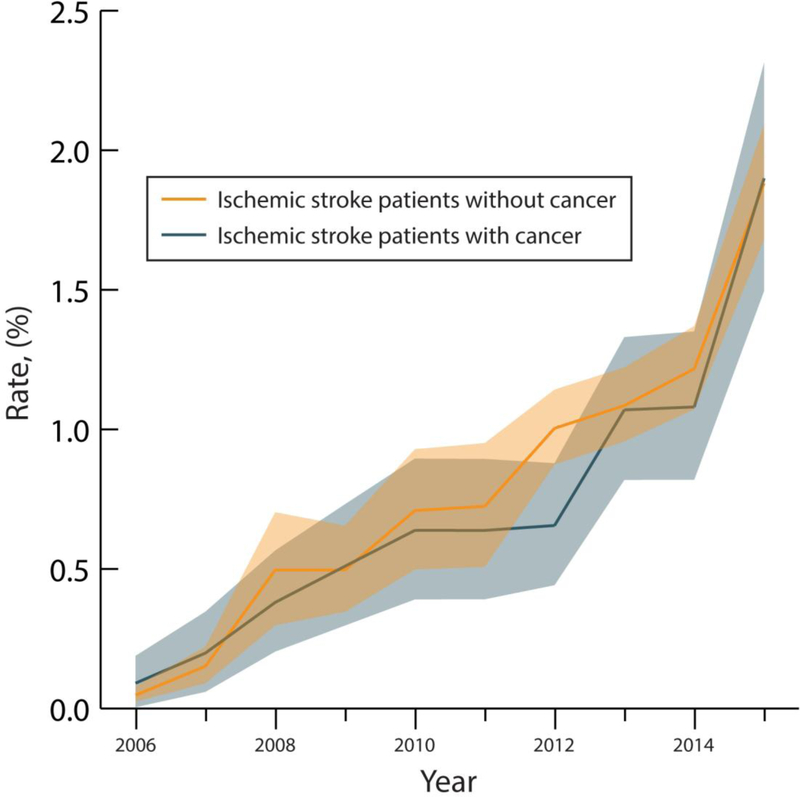
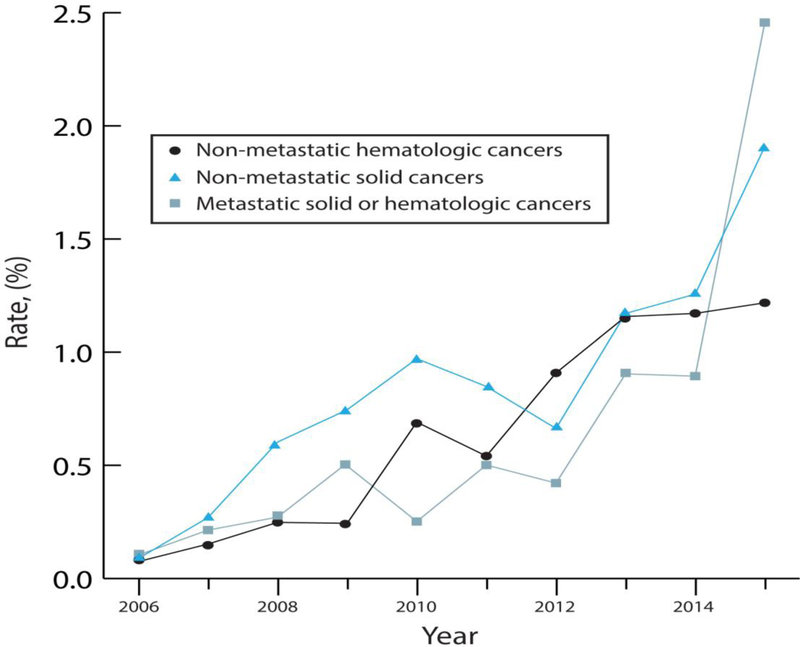
Results: Among 9,508,804 AIS hospitalizations, 503,510 (5.3%) involved cancer patients. Intravenous thrombolysis use among ischemic stroke patients with cancer increased from .01% (95% confidence interval [CI], .00%-.02%) in 1998 to 4.91% (95% CI, 4.33%-5.48%) in 2015, whereas intravenous thrombolysis use among ischemic stroke patients without cancer increased from .02% (95% CI, .01%-.02%) in 1998 to 7.22% (95% CI, 6.98%-7.45%) in 2015. The demographic- and comorbidity-adjusted odds ratio/year of receiving intravenous thrombolysis was similar in patients with cancer (1.21; 95% CI, 1.20-1.23) versus those without (1.20; 95% CI, 1.19-1.21). EVT use among ischemic stroke patients with cancer increased from .05% (95% CI, .02%-.07%) in 2006 to 1.90% (95% CI, 1.49%-2.31%) in 2015, whereas EVT use among ischemic stroke patients without cancer increased from .09% (95% CI, .00%-.18%) in 2006 to 1.88% (95% CI, 1.68%-2.09%) in 2015.
Conclusions: Among 9.5 million AIS hospitalizations, patients with cancer received intravenous thrombolysis about two thirds as often as patients without cancer. This difference persisted over time despite increased utilization in both groups. EVT utilization was similar between cancer and non-cancer AIS patients.
Keywords: Cancer; endovascular therapy; ischemic stroke; oncology; recanalization therapy; thrombolysis.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Conflicting Interests
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Sex and racial disparity in utilization and outcomes of t-PA and thrombectomy in acute ischemic stroke.J Stroke Cerebrovasc Dis. 2020 Sep;29(9):104954. doi: 10.1016/j.jstrokecerebrovasdis.2020.104954. Epub 2020 Jun 30. J Stroke Cerebrovasc Dis. 2020. PMID: 32807414
-
Preceding Intravenous Thrombolysis in Patients Receiving Endovascular Therapy.Cerebrovasc Dis. 2017;44(1-2):51-58. doi: 10.1159/000471492. Epub 2017 Apr 21. Cerebrovasc Dis. 2017. PMID: 28427054
-
Acute Ischemic Stroke Therapy in Infective Endocarditis: Case Series and Systematic Review.J Stroke Cerebrovasc Dis. 2019 Aug;28(8):2207-2212. doi: 10.1016/j.jstrokecerebrovasdis.2019.04.039. Epub 2019 May 23. J Stroke Cerebrovasc Dis. 2019. PMID: 31129109
-
Meta-analysis of the Smoker's Paradox in Acute Ischemic Stroke Patients Receiving Intravenous Thrombolysis or Endovascular Treatment.Nicotine Tob Res. 2019 Aug 19;21(9):1181-1188. doi: 10.1093/ntr/ntz094. Nicotine Tob Res. 2019. PMID: 31219582
-
Bridging versus Direct Mechanical Thrombectomy in Acute Ischemic Stroke: A Subgroup Pooled Meta-Analysis for Time of Intervention, Eligibility, and Study Design.Cerebrovasc Dis. 2020;49(2):223-232. doi: 10.1159/000507844. Epub 2020 Apr 24. Cerebrovasc Dis. 2020. PMID: 32335550
Cited by
-
Mechanical Thrombectomy for Acute Ischemic Stroke in Patients with Malignancy: A Systematic Review.J Clin Med. 2022 Aug 11;11(16):4696. doi: 10.3390/jcm11164696. J Clin Med. 2022. PMID: 36012933 Free PMC article. Review.
-
Recanalisation theraphy for acute ischemic stroke in cancer patients.Sci Rep. 2021 Jun 2;11(1):11634. doi: 10.1038/s41598-021-91257-5. Sci Rep. 2021. PMID: 34079015 Free PMC article.
-
Malignancy-associated ischemic stroke: Implications for diagnostic and therapeutic workup.CNS Neurosci Ther. 2024 Mar;30(3):e14619. doi: 10.1111/cns.14619. CNS Neurosci Ther. 2024. PMID: 38532275 Free PMC article. Review.
References
-
- Jauch EC, Saver JL, Adams HP Jr., et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013;44:870–947. - PubMed
-
- National Institute of Neurological Disorders and Stroke rt-TPA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333:1581–1587. - PubMed
-
- Berkhemer OA, Fransen PS, Beumer D, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med 2015;372:11–20. - PubMed
-
- Yeo LL, Paliwal P, Teoh HL, et al. Timing of recanalization after intravenous thrombolysis and functional outcomes after acute ischemic stroke. JAMA Neurol 2013;70:353–358. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
