

Insurance Payer Type and Patient Income Are Associated with Outcomes after Total Shoulder Arthroplasty
- PMID: 31154417
- PMCID: PMC6885106
- DOI: 10.3899/jrheum.190287
Insurance Payer Type and Patient Income Are Associated with Outcomes after Total Shoulder Arthroplasty
Abstract
Objective: To assess the independent association of insurance and patient income with total shoulder arthroplasty (TSA) outcomes.
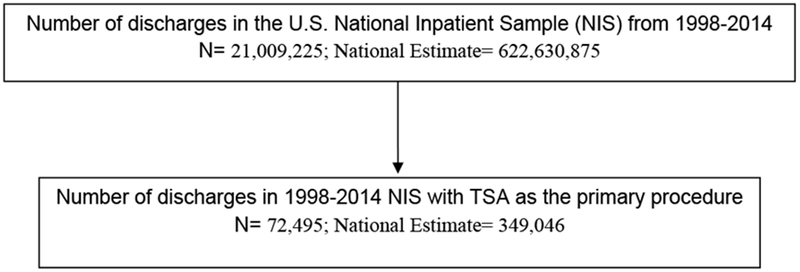
Methods: We used the 1998-2014 US National Inpatient Sample. We used multivariable-adjusted logistic regression to examine whether insurance type and the patient's median household income (based on postal code) were independently associated with healthcare use (discharge destination, hospital stay duration, total hospital charges) and in-hospital complications post-TSA based on the diagnostic codes (fracture, infection, transfusion, or revision surgery). We calculated the OR and 95% CI.
Results: Among the 349,046 projected TSA hospitalizations, the mean age was 68.6 years, 54% were female, and 73% white. Compared to private insurance, Medicaid and Medicare (government insurance) users were associated with significantly higher adjusted OR (95% CI) of (1) discharge to a rehabilitation facility, 2.16 (1.72-2.70) and 2.27 (2.04-2.52); (2) hospital stay > 2 days, 1.65 (1.45-1.87) and 1.60 (1.52-1.69); and (3) transfusion, 1.35 (1.05-1.75) and 1.39 (1.24-1.56), respectively. Medicaid was associated with a higher risk of fracture [1.74 (1.07-2.84)] and Medicare user with a higher risk of infection [2.63 (1.24-5.57)]; neither were associated with revision. Compared to the highest income quartile, the lowest income quartile was significantly associated with (OR, 95% CI): (1) discharge to a rehabilitation facility (0.89, 0.83-0.96); (2) hospital stay > 2 days (0.84, 0.80-0.89); (3) hospital charges above the median (1.19, 1.14-1.25); (4) transfusion (0.73, 0.66-0.81); and (5) revision (0.49, 0.30-0.80), but not infection or fracture.
Conclusion: This information can help to risk-stratify patients post-TSA. Future assessments of modifiable mediators of these complications are needed.
Keywords: HEALTHCARE USE; MEDICAL INSURANCE; TOTAL SHOULDER ARTHROPLASTY.
Comment in
-
Scratching the Surface: Itching for Evidence to Reduce Surgical Health Disparities in Total Shoulder Arthroplasty.J Rheumatol. 2020 Apr;47(4):490-492. doi: 10.3899/jrheum.190796. J Rheumatol. 2020. PMID: 32238543 No abstract available.
References
-
- Day JS, Lau E, Ong KL, Williams GR, Ramsey ML, Kurtz SM. Prevalence and projections of total shoulder and elbow arthroplasty in the United States to 2015. J Shoulder Elbow Surg 2010;19:1115–20. - PubMed
-
- Deshmukh AV, Koris M, Zurakowski D, Thornhill TS. Total shoulder arthroplasty: long-term survivorship, functional outcome, and quality of life. J Shoulder Elbow Surg 2005;14:471–9. - PubMed
-
- Collins DN, Harryman DT 2nd, Wirth MA. Shoulder arthroplasty for the treatment of inflammatory arthritis. J Bone Joint Surg Am 2004;86-A:2489–96. - PubMed
-
- Singh JA, Ramachandran R. Age-related differences in the use of total shoulder arthroplasty over time: use and outcomes. Bone Joint J 2015;97-B:1385–9. - PubMed
-
- Issa K, Pierce CM, Pierce TP, Boylan MR, Zikria BA, Naziri Q, et al. Total Shoulder Arthroplasty Demographics, Incidence, and Complications-A Nationwide Inpatient Sample Database Study. Surg Technol Int 2016;29:240–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials