

Characteristics, Prevention, and Management of Cardiovascular Disease in People Living With HIV: A Scientific Statement From the American Heart Association
- PMID: 31154814
- PMCID: PMC7993364
- DOI: 10.1161/CIR.0000000000000695
Characteristics, Prevention, and Management of Cardiovascular Disease in People Living With HIV: A Scientific Statement From the American Heart Association
Abstract
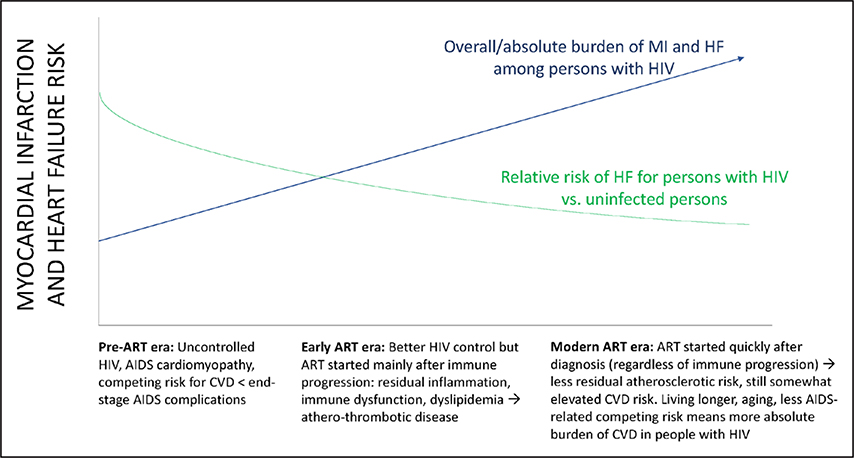
As early and effective antiretroviral therapy has become more widespread, HIV has transitioned from a progressive, fatal disease to a chronic, manageable disease marked by elevated risk of chronic comorbid diseases, including cardiovascular diseases (CVDs). Rates of myocardial infarction, heart failure, stroke, and other CVD manifestations, including pulmonary hypertension and sudden cardiac death, are significantly higher for people living with HIV than for uninfected control subjects, even in the setting of HIV viral suppression with effective antiretroviral therapy. These elevated risks generally persist after demographic and clinical risk factors are accounted for and may be partly attributed to chronic inflammation and immune dysregulation. Data on long-term CVD outcomes in HIV are limited by the relatively recent epidemiological transition of HIV to a chronic disease. Therefore, our understanding of CVD pathogenesis, prevention, and treatment in HIV relies on large observational studies, randomized controlled trials of HIV therapies that are underpowered to detect CVD end points, and small interventional studies examining surrogate CVD end points. The purpose of this document is to provide a thorough review of the existing evidence on HIV-associated CVD, in particular atherosclerotic CVD (including myocardial infarction and stroke) and heart failure, as well as pragmatic recommendations on how to approach CVD prevention and treatment in HIV in the absence of large-scale randomized controlled trial data. This statement is intended for clinicians caring for people with HIV, individuals living with HIV, and clinical and translational researchers interested in HIV-associated CVD.
Keywords: AHA Scientific Statements; HIV; cardiovascular diseases; preventive medicine.
Conflict of interest statement
The American Heart Association makes every effort to avoid any actual or potential conflicts of interest that may arise as a result of an outside relationship or a personal, professional, or business interest of a member of the writing panel. Specifically, all members of the writing group are required to complete and submit a Disclosure Questionnaire showing all such relationships that might be perceived as real or potential conflicts of interest.
Figures
References
-
- Palella FJ Jr, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, Aschman DJ, Holmberg SD. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection: HIV Outpatient Study Investigators. N Engl J Med. 1998;338:853–860. doi: 10.1056/NEJM199803263381301 - DOI - PubMed
-
- Palella FJ Jr, Baker RK, Moorman AC, Chmiel JS, Wood KC, Brooks JT, Holmberg SD; HIV Outpatient Study Investigators. Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr. 2006;43:27–34. doi: 10.1097/01.qai.0000233310.90484.16 - DOI - PubMed
-
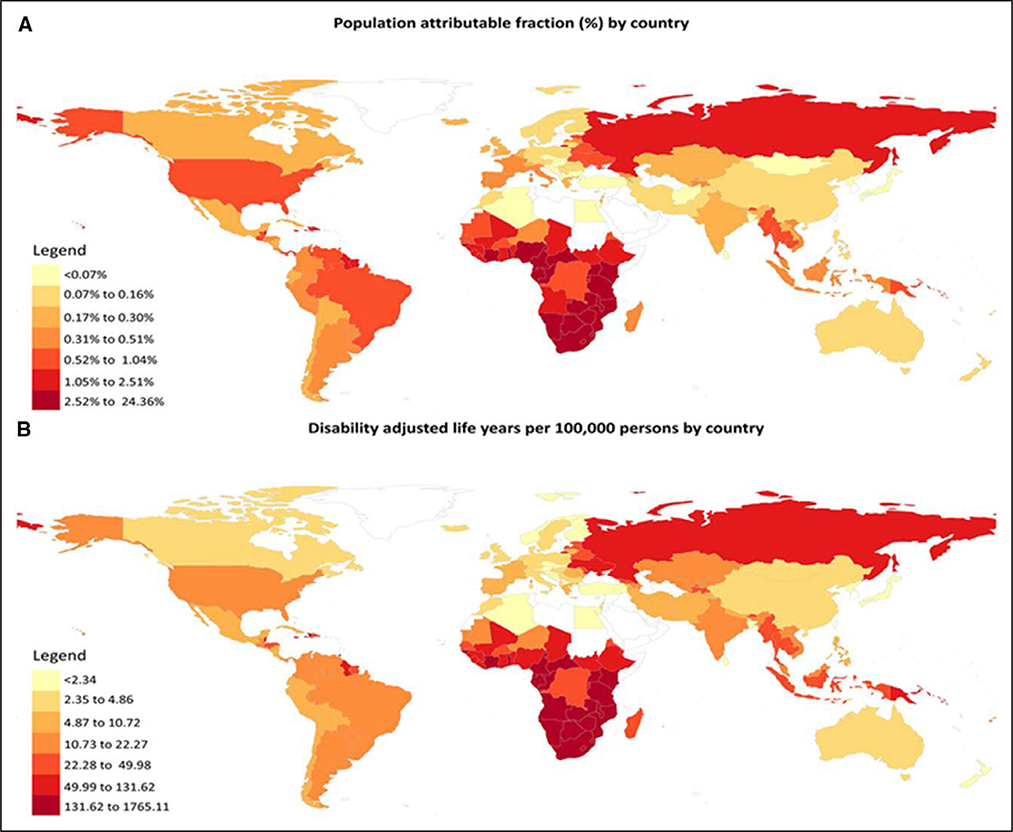
- Shah ASV, Stelzle D, Lee KK, Beck EJ, Alam S, Clifford S, Longenecker CT, Strachan F, Bagchi S, Whiteley W, Rajagopalan S, Kottilil S, Nair H, Newby DE, McAllister DA, Mills NL. Global burden of atherosclerotic cardiovascular disease in people living with the HIV: a systematic review and meta-analysis. Circulation. 2018;138:1100–1112. doi: 10.1161/CIRCULATIONAHA.117.033369 - DOI - PMC - PubMed
-
- Freiberg MS, Chang CC, Kuller LH, Skanderson M, Lowy E, Kraemer KL, Butt AA, Bidwell Goetz M, Leaf D, Oursler KA, Rimland D, Rodriguez Barradas M, Brown S, Gibert C, McGinnis K, Crothers K, Sico J, Crane H, Warner A, Gottlieb S, Gottdiener J, Tracy RP, Budoff M, Watson C, Armah KA, Doebler D, Bryant K, Justice AC. HIV infection and the risk of acute myocardial infarction. JAMA Intern Med. 2013;173:614–622. doi: 10.1001/jamainternmed.2013.3728 - DOI - PMC - PubMed
