

Realizing the right to health in Brazil's Unified Health System through the lens of breast and cervical cancer
- PMID: 31155002
- PMCID: PMC6545675
- DOI: 10.1186/s12939-019-0938-x
Realizing the right to health in Brazil's Unified Health System through the lens of breast and cervical cancer
Abstract
Background: Health is recognized as a fundamental right in Brazil's constitution. In the absence of a clearly defined benefit packages of healthcare services that are financed under the Unified Health System (Sistema Único de Saúde, SUS), courts have become important in adjudicating coverage decisions. Empirical assessments of equity and the right to health tend to focus on simple measures of access. However, these empirical perspectives belie the significant inequalities and rights violations that arise in the case of more complex health needs such as cancer. To shed light on these issues, this paper focuses on the care pathways for breast and cervical cancer and explores access and quality issues that arise at different points along the care pathway with implications for the realization of the right to health in Brazil.
Method: A mixed method approach is used. The analysis is primarily based on a quantitative analysis of national representative administrative data principally from the cervical and breast cancer information systems and the hospital cancer registry. To gain more insights into the organization of cancer care, qualitative data was collected from the state of Bahia, through document analysis, direct observation, roundtable discussions with health workers (HWs), and structured interviews with health care administrators.
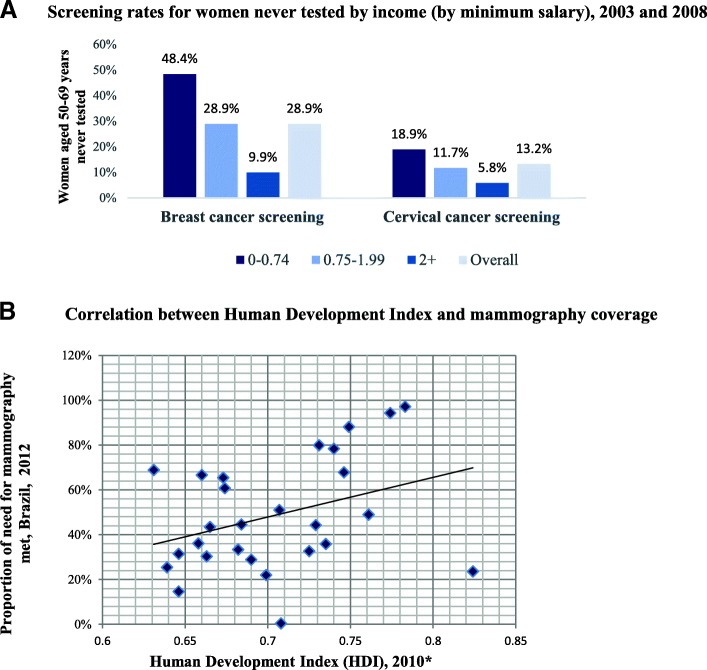
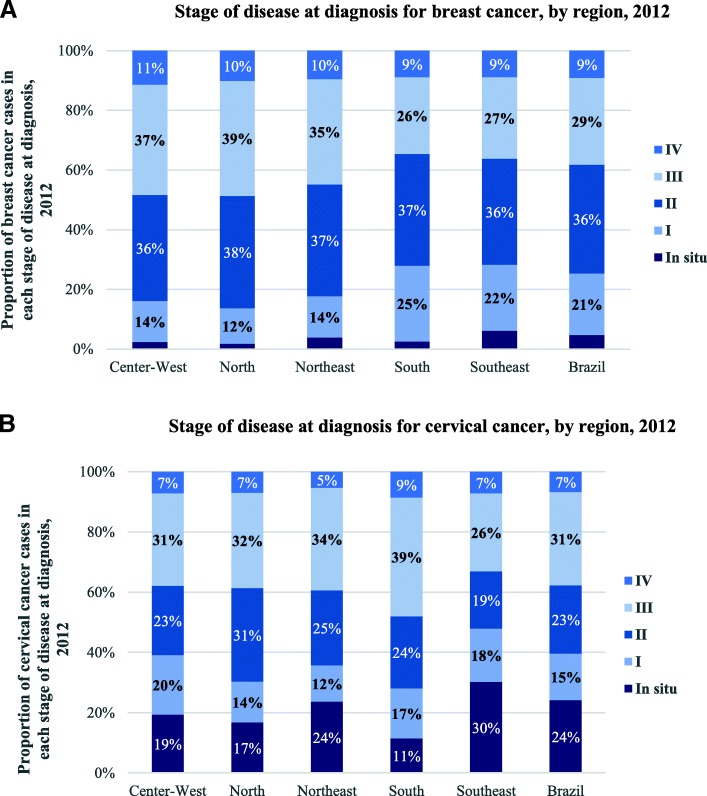
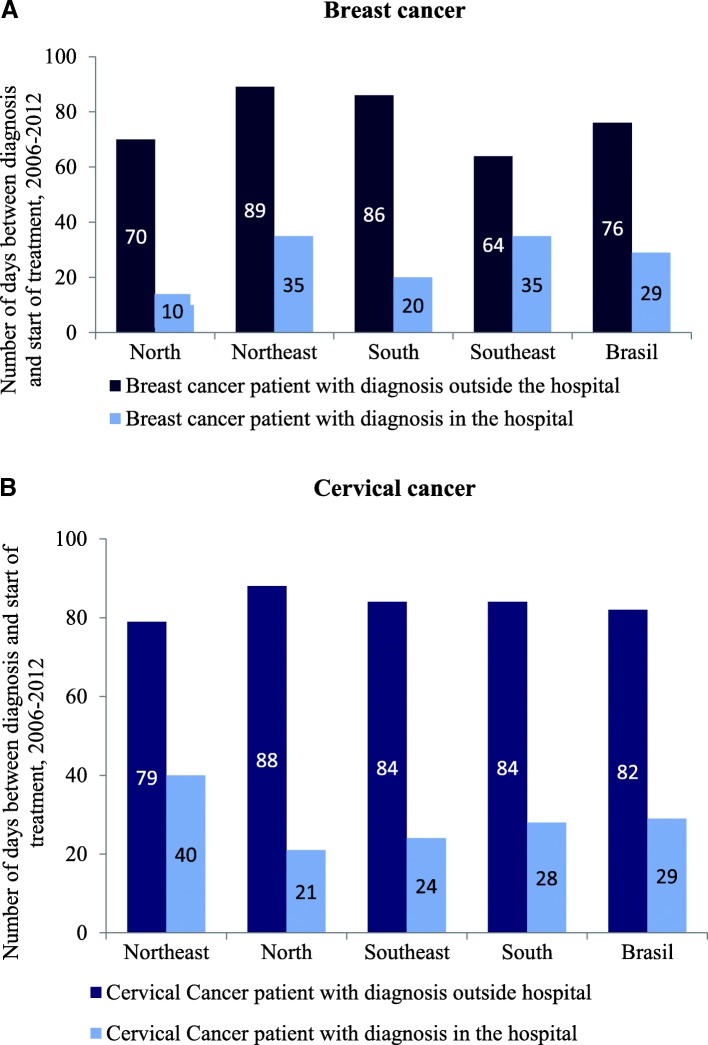
Results: The paper reveals that the volume of completed screening exams is well below the estimated need, and a tendency toward lower breast cancer screening rates in poorer states and for women in the lowest income brackets. Only 26% of breast cancer cases and 29% of cervical cancer cases are diagnosed at an early stage (stage 0 or I), thereby reducing the survival prospects of patients. Waiting times between confirmed diagnosis and treatment are long, despite new legislation that guarantees a maximum of 60 days. The waiting times are significantly longer for patients that follow the recommended patient pathways, and who are diagnosed outside the hospital.
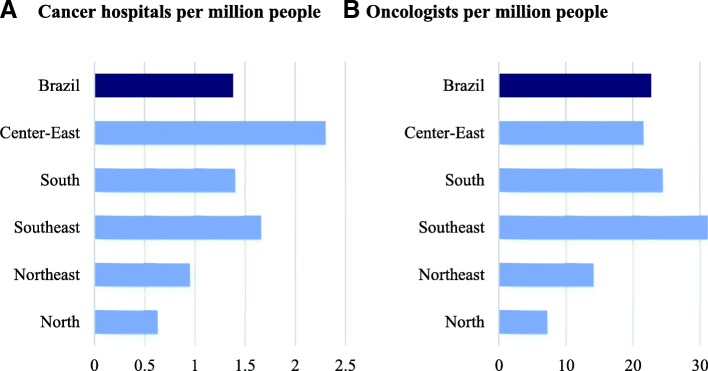
Conclusion: The study reveals that there are large variations between states and patients, where the poorest states and patients fare worse on key indicators. More broadly, the paper shows the importance of collecting data both on patient characteristics and health system performance and carry out detailed health system analysis for exposing, empirically, rights violations and for identifying how they can be addressed.
Keywords: Bahia; Brazil; Brazil’s Unified Health System (Sistema Único de Saúde, SUS); Breast cancer; Cancer care; Cervical cancer; Equity; Health system; Right to health.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Yamin AE. Taking the right to Health seriously: implications for Health systems, courts, and achieving universal Health coverage. Hum Rights Q. 2017;39(2):341–368. doi: 10.1353/hrq.2017.0021. - DOI
-
- WHO. Making fair choices on the path to universal health coverage: Final report of the WHO consultative group on equity and universal Health coverage. Geneva: World Health Organization. 2014. http://apps.who.int/iris/bitstream/10665/112671/1/9789241507158_eng.pdf?.... Accessed 30 Apr 2018.
-
- WHO. Positioning health in the post-2015 development agenda. WHO discussion paper. October 2012. http://www.who.int/topics/millennium_development_goals/post2015/WHOdiscu.... Accessed 30 Apr 2018.
-
- WHO. Constitution of the World Health Organization as adopted by the International Health Conference, New York 19–22 June, 1946; signed on 22 July 1946 by the representatives of 61 States (Official Records of the World Health Organization no 2).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
