

Epilepsy and Neurodevelopmental Outcomes in Children With Etiologically Diagnosed Central Nervous System Infections: A Retrospective Cohort Study
- PMID: 31156546
- PMCID: PMC6529952
- DOI: 10.3389/fneur.2019.00528
Epilepsy and Neurodevelopmental Outcomes in Children With Etiologically Diagnosed Central Nervous System Infections: A Retrospective Cohort Study
Abstract
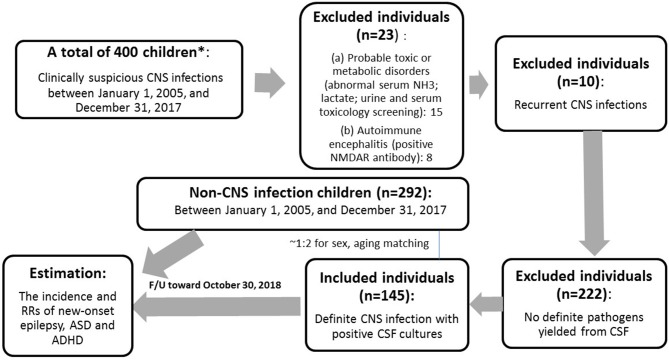
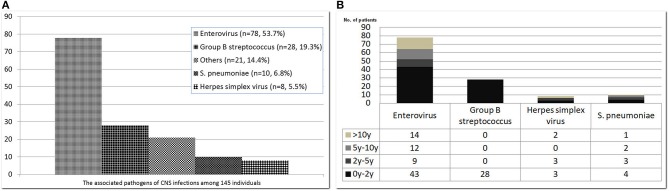
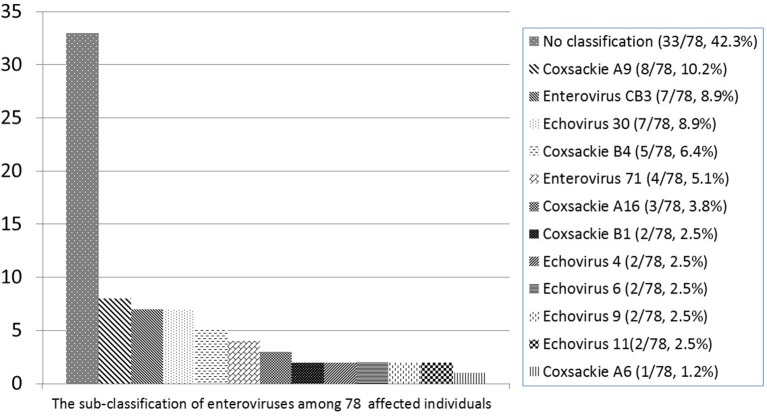
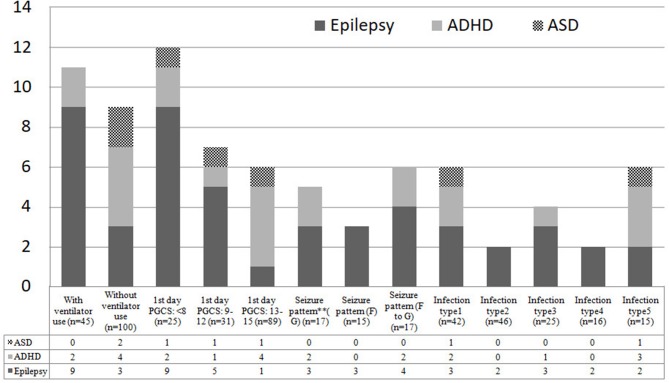
Background: Central nervous system (CNS) infection in childhood can lead to neurological sequelae, including epilepsy, and neurodevelopmental disorders, such as attention-deficit/hyperactivity disorder (ADHD) and autism spectrum disorder (ASD). This study investigated the association of etiologically diagnosed childhood brain infections with the subsequent risks of epilepsy and neurodevelopmental disorders. Objectives: We retrospectively analyzed the data of children aged <18 years who had definite brain infections with positive cerebrospinal fluid cultures from January 1, 2005, to December 31, 2017. These patients were followed to evaluate the risks of epilepsy and neurodevelopmental disease (ADHD and ASD) after brain infections (group 1) in comparison with the risks in those without brain infections (group 2). Results: A total of 145 patients with an average age of 41.2 months were included in group 1. Enterovirus accounted for the majority of infections, followed by group B Streptococcus, S. pneumoniae, and herpes simplex virus. A total of 292 patients with an average age of 44.8 months were included in group 2. The 12-year risk of epilepsy in group 1 was 10.7 (95% confidence interval [CI], 2.30-49; p < 0.01). Compared with group 2 (reference), the risk of ASD in the age interval of 2-5 years in group 1 was 21.3 (95% CI, 1.33-341.4; p = 0.03). The incidence of ADHD in group 1 was not significantly higher than that in group 2. Conclusions: This study identified the common etiological causes of brain infections in Taiwanese children. The highest-risk neurodevelopmental sequelae associated with brain infections was epilepsy. Children who had a diagnosis of brain infection (specially Enterovirus) should be followed since they are at greater risk of developing epilepsy and ASD.
Keywords: brain infections; central nervous system infections; children; epilepsy; neurodevelopmental outcomes.
Figures
References
-
- Annegers JF, Hauser WA, Beghi E, Nicolosi A, Kurland LT. The risk of unprovoked seizures after encephalitis and meningitis. Neurology. (1988) 38:1407–10. - PubMed
-
- Arditi M, Mason EO, Jr, Bradley JS, Tan TQ, Barson WJ, Schutze GE, et al. Three-year multicenter surveillance of pneumococcal meningitis in children: clinical characteristics, and outcome related to penicillin susceptibility and dexamethasone use. Pediatrics. (1998) 102:1087–97. - PubMed
-
- Pomeroy SL, Holmes SJ, Dodge PR, Feigin RD. Seizures and other neurologic sequelae of bacterial meningitis in children. N Engl J Med. (1990) 323:1651–7. - PubMed
LinkOut - more resources
Full Text Sources