

Impact of clinical pharmacist intervention on length of stay in an acute admission unit: a cluster randomised study
- PMID: 31156841
- PMCID: PMC6451522
- DOI: 10.1136/ejhpharm-2015-000767
Impact of clinical pharmacist intervention on length of stay in an acute admission unit: a cluster randomised study
Abstract
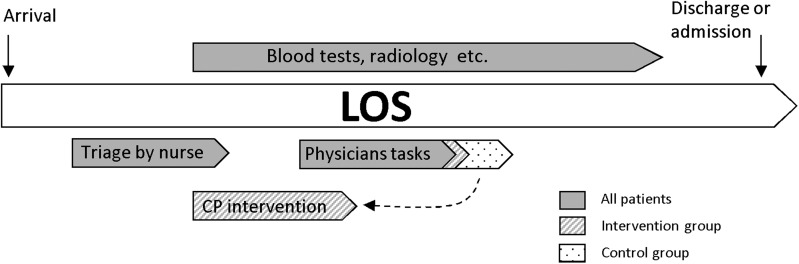
Objectives: Physicians in acute admission units (AAUs) are obliged to obtain medication history and perform medication reconciliation, which is time consuming and often incomplete. Studies show that clinical pharmacists (CPs) can obtain accurate medication histories, but so far no studies have investigated the effect of this on time measures. Therefore, the objective of the present study was to investigate the effect of a CP intervention on length of stay (LOS) in an AAU.
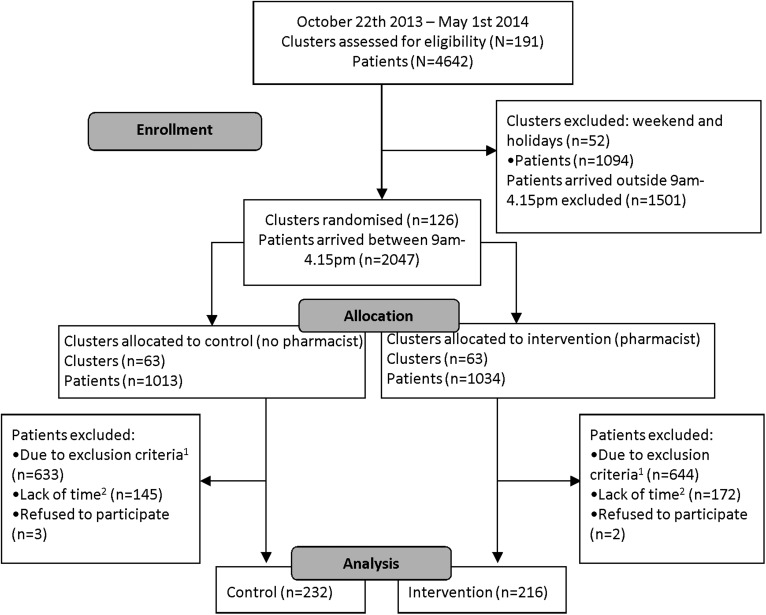
Methods: The study was designed as a prospective, cluster randomised study. Weekdays were randomised to control or intervention. CP intervention consisted of obtaining medication history and performing medication reconciliation and review. The primary outcome was LOS in the AAU. Secondary outcomes were other time-related measures-for example, physicians' self-reported time spent on medication topics. Finally, the number of documented medications per patient was established.
Results: 232 and 216 patients, respectively, were included on control (n=63) and intervention (n=63) days. The mean LOS was 342 (95% CI 323 to 362) min in the intervention group and 339 (95% CI 322 to 357) min in the control group, which was not statistically significantly different. Physicians spent on average 4.3 (95% CI 3.7 to 5.0) min in the intervention group and 7.5 (95% CI 6.6 to 8.5) min in the control group, corresponding to an overall reduction of 43.0% (95% CI 30.9% to 53.0%, p<0.001). The number of documented medications per patient was 10.0 (intervention group) and 8.8 (control group).
Conclusions: This study indicates that LOS in the AAU was not affected by CP intervention; however, physicians reported a significant reduction in time spent on medication topics.
Trial registration number: Clinical Trial Gov: 1-16-02-379-13.
Keywords: ACCIDENT & EMERGENCY MEDICINE; CLINICAL PHARMACY; Length of stay; acute admission unit; medication history conduction; medication reconcilliation; medication review.
Conflict of interest statement
Competing interests: None declared.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous