

A 28-Year-Old Woman with Ascites and Multiple Focal Spleen Lesions
- PMID: 31157180
- PMCID: PMC6542493
- DOI: 10.12890/2019_001061
A 28-Year-Old Woman with Ascites and Multiple Focal Spleen Lesions
Abstract
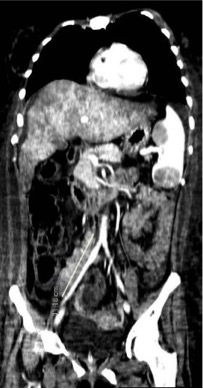
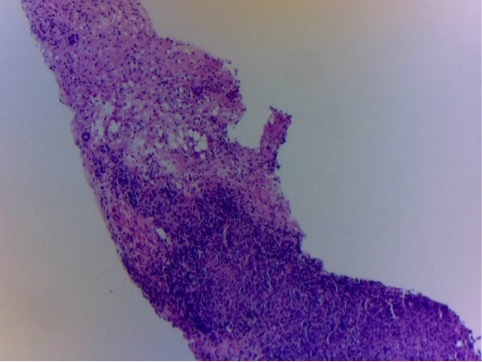
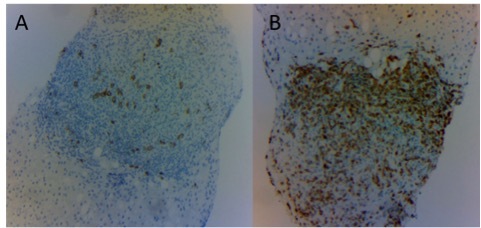
Serous effusions complicating the course of lymphomas occur commonly in the pleural space but seldom in the peritoneum, where they most often present as chylous ascites with diagnostic cytology. Almost invariably, in these rare cases, the serum to ascites albumin gradient is low. We describe a 28-year-old woman with anasarca, ascites and a serum to ascites albumin gradient of 1.1 g/dl, consistent with portal hypertension. No tumour cells were detected in the ascitic fluid. However, a CT scan of the chest and abdomen disclosed liver and spleen enlargement and multiple enlarged retroperitoneal lymph nodes, suspicious for a lymphoproliferative disorder. Bone marrow aspiration and biopsy were not diagnostic, so a decision was made to proceed with a splenectomy despite the onset of low-grade disseminated intravascular coagulation. Surgery was uneventful. Diffuse large B cell lymphoma was diagnosed. A liver biopsy taken at the time of surgery demonstrated that the liver parenchyma was massively infiltrated by reactive T lymphocytes surrounding rare large CD20+ tumour cells. This infiltrate had likely led to increased portal pressure attended by ascites formation, which resolved completely after chemotherapy. The case emphasizes the rewards of pursuing a diagnosis supported by a high prior probability even in the presence of apparently discordant laboratory findings, as well as the importance of performing a diagnostic splenectomy in case of splenomegaly with unexplained focal lesions.
Learning points: Lymphomas may present with serous effusion, which is usually chylous and with positive cytology when represented by ascites accumulation; non-chylous effusions can be due to altered lymphatic drainage, extrinsic compression of the portal vein by enlarged lymph nodes as well as massive infiltration of the liver by lymphoma.If the cause of splenomegaly is unclear, diagnostic splenectomy remains a viable option.The diagnosis of lymphoma should always be pursued, even if it requires apparently unwise surgery, since this type of cancer can be treated effectively only if thoroughly characterized pathologically and molecularly.
Keywords: Ascites; diagnostic splenectomy; disseminated intravascular coagulation; lymphoma; splenomegaly.
Conflict of interest statement
Conflicts of Interests: The Authors declare that there are no competing interests.
Figures



References
-
- Runyon BA. Management of adult patients with ascites due to cirrhosis. Hepatology. 2004;39:841–856. - PubMed
-
- Riquelme A, Calvo M, Salech F, Valderrama S, Pattillo A, Arellano M, et al. Value of adenosine deaminase (ADA) in ascitic fluid for the diagnosis of tuberculous peritonitis: a meta-analysis. J Clin Gastroenterol. 2006;40:705–710. - PubMed
-
- Schouten JN, Garcia-Pagan JC, Valla DC, Janssen HL. Idiopathic noncirrhotic portal hypertension. Hepatology. 2011;54:1071–1081. - PubMed
-
- Das DK. Serous effusions in malignant lymphomas: a review. Diagn Cytopathol. 2006;34:335–347. - PubMed
-
- Almakdisi T, Massoud S, Makdisi G. Lymphomas and chylous ascites: review of the literature. Oncologist. 2005;10:632–635. - PubMed
LinkOut - more resources
Full Text Sources