

Persistent neuropathological effects 14 years following amyloid-β immunization in Alzheimer's disease
- PMID: 31157360
- PMCID: PMC6598630
- DOI: 10.1093/brain/awz142
Persistent neuropathological effects 14 years following amyloid-β immunization in Alzheimer's disease
Abstract
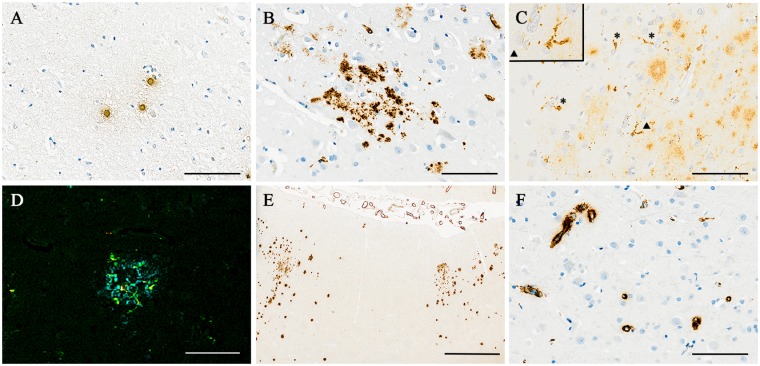
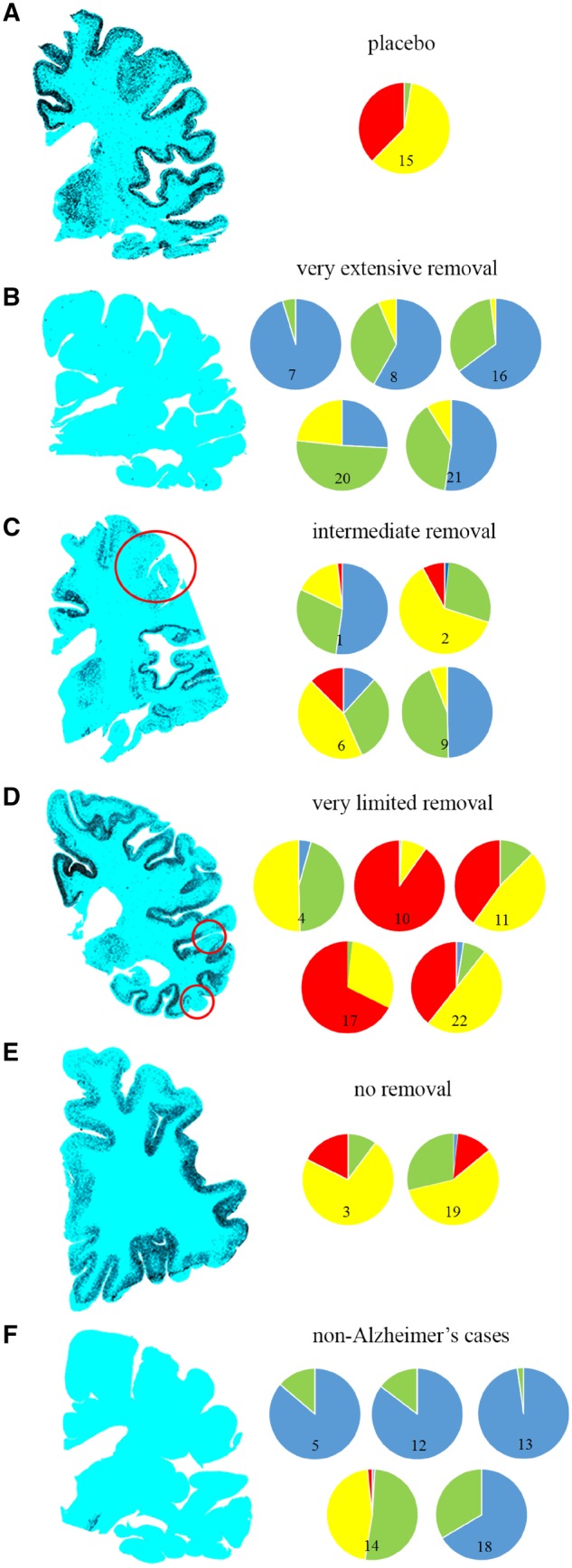
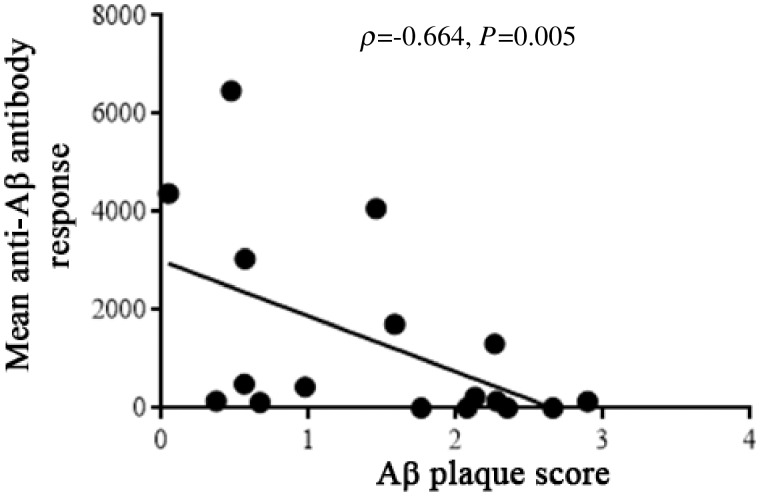
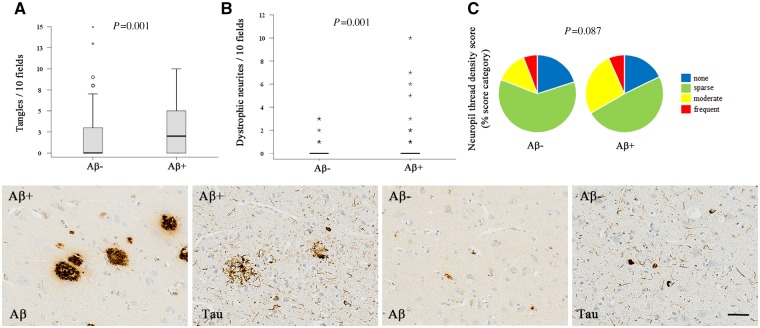
We performed a 15-year post-mortem neuropathological follow-up of patients in the first trial of amyloid-β immunotherapy for Alzheimer's disease. Twenty-two participants of a clinical trial of active amyloid-β42 immunization (AN1792, Elan Pharmaceuticals) or placebo were studied. Comprehensive post-mortem neuropathological assessments were performed from 4 months to 15 years after the trial. We analysed the relationships between the topographical distribution of amyloid-β removal from the cerebral cortex and tau pathology, cerebrovascular territories, plasma anti-AN1792 antibody titres and late cognitive status. Seventeen of 22 (77%) participants had Alzheimer's neuropathological change, whereas 5 of 22 (23%) had alternative causes for dementia (progressive supranuclear palsy = 1, Lewy body disease = 1, vascular brain injury = 1, and frontotemporal lobar degeneration = 2). Nineteen of the 22 participants had received the active agent, three the placebo. Fourteen of 16 (88%) patients with Alzheimer's disease receiving the active agent had evidence of plaque removal (very extensive removal = 5, intermediate = 4, very limited = 5, no removal = 2). Of particular note, two Alzheimer's patients who died 14 years after immunization had only very sparse or no detectable plaques in all regions examined. There was a significant inverse correlation between post-vaccination peripheral blood anti-AN1792 antibody titres and post-mortem plaque scores (ρ = - 0.664, P = 0.005). Cortical foci cleared of plaques contained less tau than did cortex with remaining plaques, but the overall distribution of tangles was extensive (Braak V/VI). In conclusion, patients with Alzheimer's disease actively immunized against amyloid-β can remain virtually plaque-free for 14 years. The extent of plaque removal is related to the immune response. This long duration of efficacy is important in support of active immunization protocols as therapy for, or potentially prevention of, neurodegeneration-associated protein accumulations. Inclusion of patients without Alzheimer's disease in Alzheimer's therapy trials is a problem for assessing the efficacy of treatment. Despite modification of Alzheimer's pathology, most patients had progressed to severe dementia, notably including the five with very extensive plaque removal, possibly due to continued tau propagation. Neuropathology follow-up of patients in therapeutic trials provides valuable information on the causes of dementia and effects of treatment.
Keywords: Alzheimer’s disease; amyloid-β; dementia; immunotherapy; neuropathology.
© The Author(s) (2019). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
Comment in
-
Could changing the course of Alzheimer's disease pathology with immunotherapy prevent dementia?Brain. 2019 Jul 1;142(7):1853-1855. doi: 10.1093/brain/awz165. Brain. 2019. PMID: 31505546 Free PMC article.
References
-
- Amin J, Paquet C, Baker A, Asuni AA, Love S, Holmes C, et al.Effect of amyloid-beta (Abeta) immunization on hyperphosphorylated tau: a potential role for glycogen synthase kinase (GSK)-3beta. Neuropathol Appl Neurobiol 2015; 41: 445–57. - PubMed
-
- Bayer AJ, Bullock R, Jones RW, Wilkinson D, Paterson KR, Jenkins L, et al.Evaluation of the safety and immunogenicity of synthetic Abeta42 (AN1792) in patients with AD. Neurology 2005; 64: 94–101. - PubMed
-
- Boche D, Denham N, Holmes C, Nicoll JA. Neuropathology after active Abeta42 immunotherapy: implications for Alzheimer’s disease pathogenesis. Acta Neuropathol 2010a; 120: 369–84. - PubMed
-
- Boche D, Donald J, Love S, Harris S, Neal JW, Holmes C, et al.Reduction of aggregated Tau in neuronal processes but not in the cell bodies after Abeta42 immunisation in Alzheimer’s disease. Acta Neuropathol 2010b; 120: 13–20. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
