

Effect of Intraoperative High Positive End-Expiratory Pressure (PEEP) With Recruitment Maneuvers vs Low PEEP on Postoperative Pulmonary Complications in Obese Patients: A Randomized Clinical Trial
- PMID: 31157366
- PMCID: PMC6582260
- DOI: 10.1001/jama.2019.7505
Effect of Intraoperative High Positive End-Expiratory Pressure (PEEP) With Recruitment Maneuvers vs Low PEEP on Postoperative Pulmonary Complications in Obese Patients: A Randomized Clinical Trial
Erratum in
-
Incorrect and Omitted Names for Collaborators.JAMA. 2019 Nov 12;322(18):1829-1830. doi: 10.1001/jama.2019.16415. JAMA. 2019. PMID: 31714970 Free PMC article. No abstract available.
Abstract
Importance: An intraoperative higher level of positive end-expiratory positive pressure (PEEP) with alveolar recruitment maneuvers improves respiratory function in obese patients undergoing surgery, but the effect on clinical outcomes is uncertain.
Objective: To determine whether a higher level of PEEP with alveolar recruitment maneuvers decreases postoperative pulmonary complications in obese patients undergoing surgery compared with a lower level of PEEP.
Design, setting, and participants: Randomized clinical trial of 2013 adults with body mass indices of 35 or greater and substantial risk for postoperative pulmonary complications who were undergoing noncardiac, nonneurological surgery under general anesthesia. The trial was conducted at 77 sites in 23 countries from July 2014-February 2018; final follow-up: May 2018.
Interventions: Patients were randomized to the high level of PEEP group (n = 989), consisting of a PEEP level of 12 cm H2O with alveolar recruitment maneuvers (a stepwise increase of tidal volume and eventually PEEP) or to the low level of PEEP group (n = 987), consisting of a PEEP level of 4 cm H2O. All patients received volume-controlled ventilation with a tidal volume of 7 mL/kg of predicted body weight.
Main outcomes and measures: The primary outcome was a composite of pulmonary complications within the first 5 postoperative days, including respiratory failure, acute respiratory distress syndrome, bronchospasm, new pulmonary infiltrates, pulmonary infection, aspiration pneumonitis, pleural effusion, atelectasis, cardiopulmonary edema, and pneumothorax. Among the 9 prespecified secondary outcomes, 3 were intraoperative complications, including hypoxemia (oxygen desaturation with Spo2 ≤92% for >1 minute).
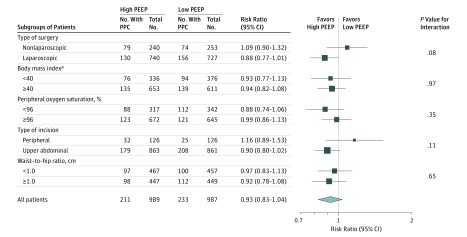
Results: Among 2013 adults who were randomized, 1976 (98.2%) completed the trial (mean age, 48.8 years; 1381 [69.9%] women; 1778 [90.1%] underwent abdominal operations). In the intention-to-treat analysis, the primary outcome occurred in 211 of 989 patients (21.3%) in the high level of PEEP group compared with 233 of 987 patients (23.6%) in the low level of PEEP group (difference, -2.3% [95% CI, -5.9% to 1.4%]; risk ratio, 0.93 [95% CI, 0.83 to 1.04]; P = .23). Among the 9 prespecified secondary outcomes, 6 were not significantly different between the high and low level of PEEP groups, and 3 were significantly different, including fewer patients with hypoxemia (5.0% in the high level of PEEP group vs 13.6% in the low level of PEEP group; difference, -8.6% [95% CI, -11.1% to 6.1%]; P < .001).
Conclusions and relevance: Among obese patients undergoing surgery under general anesthesia, an intraoperative mechanical ventilation strategy with a higher level of PEEP and alveolar recruitment maneuvers, compared with a strategy with a lower level of PEEP, did not reduce postoperative pulmonary complications.
Trial registration: ClinicalTrials.gov Identifier: NCT02148692.
Conflict of interest statement
Figures

Comment in
-
Setting Positive End-Expiratory Pressure in Mechanically Ventilated Patients Undergoing Surgery.JAMA. 2019 Jun 18;321(23):2285-2287. doi: 10.1001/jama.2019.7540. JAMA. 2019. PMID: 31157358 No abstract available.
-
Positive end expiratory pressure (PEEP) in the operative theatre: What's next?Anaesth Crit Care Pain Med. 2019 Oct;38(5):435-437. doi: 10.1016/j.accpm.2019.09.006. Anaesth Crit Care Pain Med. 2019. PMID: 31585762 No abstract available.
-
Intraoperative Ventilation Strategies to Reduce Pulmonary Complications in Obese Patients.JAMA. 2019 Nov 12;322(18):1828. doi: 10.1001/jama.2019.14394. JAMA. 2019. PMID: 31714980 No abstract available.
References
-
- Ball L, Hemmes SNT, Serpa Neto A, et al. ; Las Vegas Investigators; PROVE Network; Clinical Trial Network of the European Society of Anaesthesiology . Intraoperative ventilation settings and their associations with postoperative pulmonary complications in obese patients. Br J Anaesth. 2018;121(4):899-908. doi: 10.1016/j.bja.2018.04.021 - DOI - PubMed
-
- Fernandez-Bustamante A, Frendl G, Sprung J, et al. Postoperative pulmonary complications, early mortality, and hospital stay following noncardiothoracic surgery: a multicenter study by the Perioperative Research Network Investigators. JAMA Surg. 2017;152(2):157-166. doi: 10.1001/jamasurg.2016.4065 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
