

Association of Amyloid and Tau With Cognition in Preclinical Alzheimer Disease: A Longitudinal Study
- PMID: 31157827
- PMCID: PMC6547132
- DOI: 10.1001/jamaneurol.2019.1424
Association of Amyloid and Tau With Cognition in Preclinical Alzheimer Disease: A Longitudinal Study
Erratum in
-
Error in Figure 3.JAMA Neurol. 2019 Aug 1;76(8):986. doi: 10.1001/jamaneurol.2019.2144. JAMA Neurol. 2019. PMID: 31403691 Free PMC article. No abstract available.
Abstract
Importance: Positron emission tomography (PET) imaging now allows in vivo visualization of both neuropathologic hallmarks of Alzheimer disease (AD): amyloid-β (Aβ) plaques and tau neurofibrillary tangles. Observing their progressive accumulation in the brains of clinically normal older adults is critically important to understand the pathophysiologic cascade leading to AD and to inform the choice of outcome measures in prevention trials.
Objective: To assess the associations among Aβ, tau, and cognition, measured during different observation periods for 7 years.
Design, setting, and participants: Prospective cohort study conducted between 2010 and 2017 at the Harvard Aging Brain Study, Boston, Massachusetts. The study enrolled 279 clinically normal participants. An additional 90 individuals were approached but declined the study or did not meet the inclusion criteria. In this report, we analyzed data from 60 participants who had multiple Aβ and tau PET observations available on October 31, 2017.
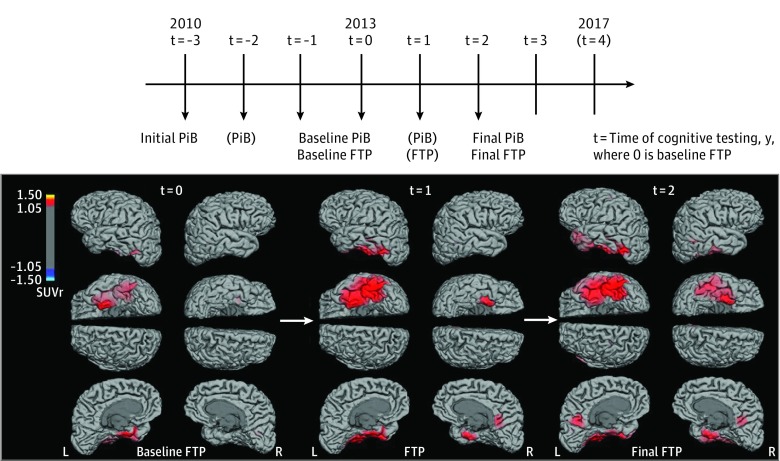
Main outcomes and measures: A median of 3 Pittsburgh compound B-PET (Aβ, 2010-2017) and 2 flortaucipir-PET (tau, 2013-2017) images were collected. We used initial PET and slope data, assessing the rates of change in Aβ and tau, to measure cognitive changes. Cognition was evaluated annually using the Preclinical Alzheimer Cognitive Composite (2010-2017). Annual consensus meetings evaluated progression to mild cognitive impairment.
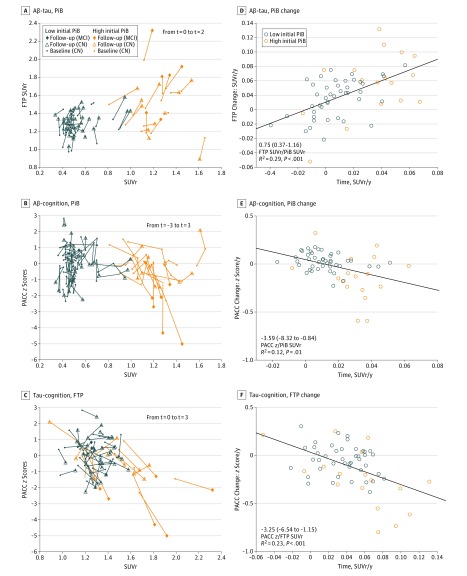
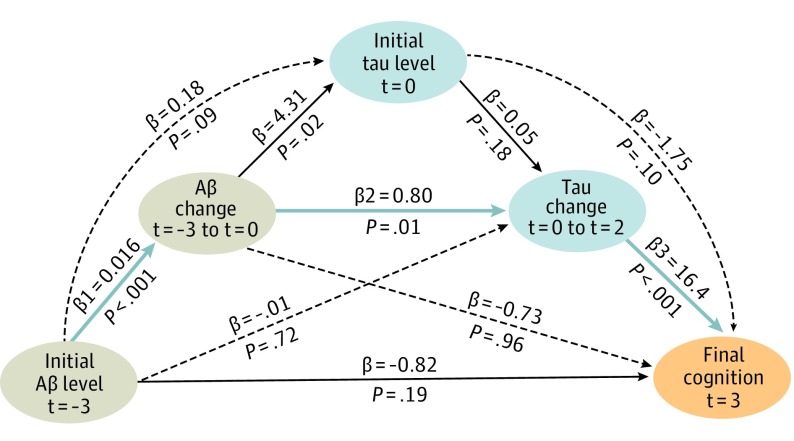
Results: Of the 60 participants, 35 were women (58%) and 25 were men (42%); median age at inclusion was 73 years (range, 65-85 years). Seventeen participants (28%) exhibited an initial high Aβ burden. An antecedent rise in Aβ was associated with subsequent changes in tau (1.07 flortaucipir standardized uptake value ratios [SUVr]/PiB-SUVr; 95% CI, 0.13-3.46; P = .02). Tau changes were associated with cognitive changes (-3.28 z scores/SUVR; 95% CI, -6.67 to -0.91; P = .001), covarying baseline Aβ and tau. Tau changes were greater in the participants who progressed to mild cognitive impairment (n = 6) than in those who did not (n = 11; 0.05 SUVr per year; 95% CI, 0.03-0.07; P = .001). A serial mediation model demonstrated that the association between initial Aβ and final cognition, measured 7 years later, was mediated by successive changes in Aβ and tau.
Conclusions and relevance: We identified sequential changes in normal older adults, from Aβ to tau to cognition, after which the participants with high Aβ with greater tau increase met clinical criteria for mild cognitive impairment. These findings highlight the importance of repeated tau-PET observations to track disease progression and the importance of repeated amyloid-PET observations to detect the earliest AD pathologic changes.
Conflict of interest statement
Figures
Comment in
-
Sequential amyloid-β and tau accumulation foreshadows cognitive decline.Nat Rev Neurol. 2019 Aug;15(8):433. doi: 10.1038/s41582-019-0230-0. Nat Rev Neurol. 2019. PMID: 31217578 No abstract available.
References
-
- McKhann GM, Knopman DS, Chertkow H, et al. . The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):263-269. doi:10.1016/j.jalz.2011.03.005 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
