

Clinical and Genomic Risk to Guide the Use of Adjuvant Therapy for Breast Cancer
- PMID: 31157962
- PMCID: PMC6709671
- DOI: 10.1056/NEJMoa1904819
Clinical and Genomic Risk to Guide the Use of Adjuvant Therapy for Breast Cancer
Abstract
Background: The use of adjuvant chemotherapy in patients with breast cancer may be guided by clinicopathological factors and a score based on a 21-gene assay to determine the risk of recurrence. Whether the level of clinical risk of breast cancer recurrence adds prognostic information to the recurrence score is not known.
Methods: We performed a prospective trial involving 9427 women with hormone-receptor-positive, human epidermal growth factor receptor 2-negative, axillary node-negative breast cancer, in whom an assay of 21 genes had been performed, and we classified the clinical risk of recurrence of breast cancer as low or high on the basis of the tumor size and histologic grade. The effect of clinical risk was evaluated by calculating hazard ratios for distant recurrence with the use of Cox proportional-hazards models. The initial endocrine therapy was tamoxifen alone in the majority of the premenopausal women who were 50 years of age or younger.
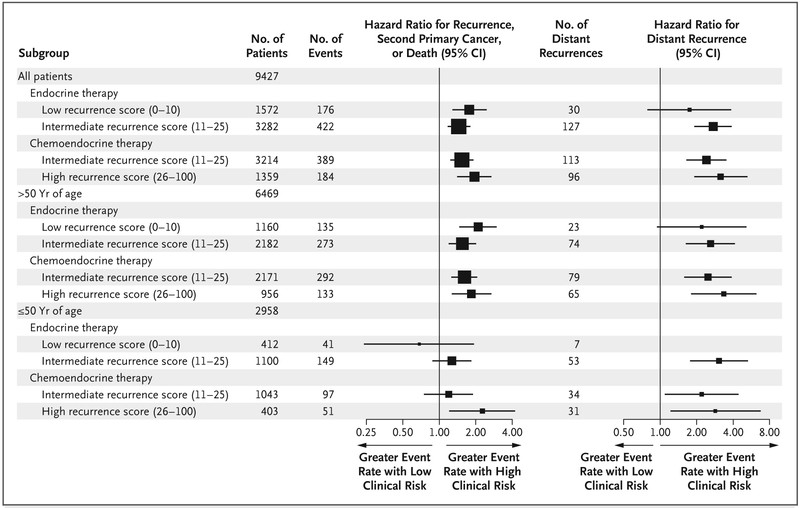
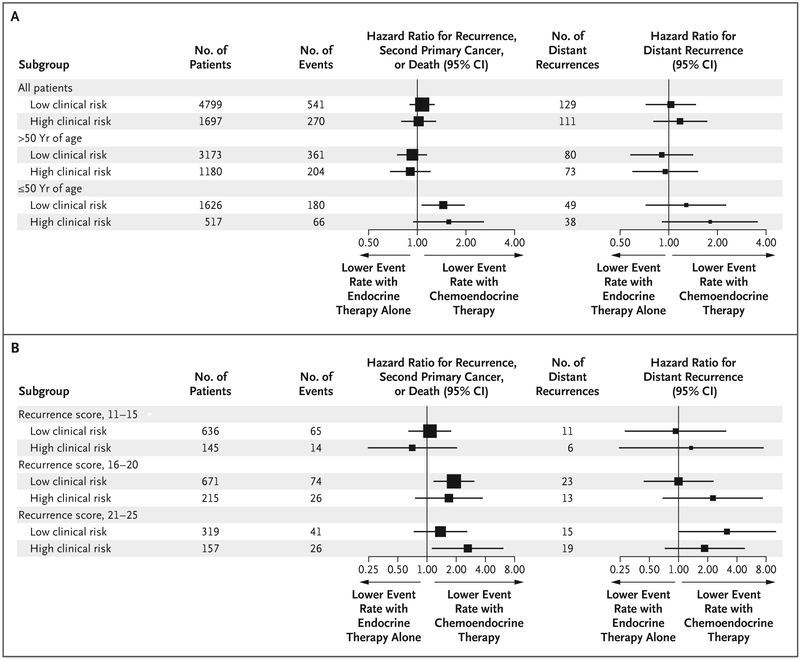
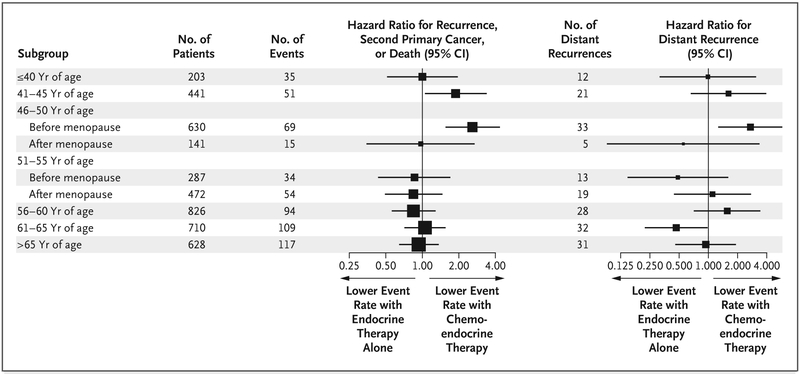
Results: The level of clinical risk was prognostic of distant recurrence in women with an intermediate 21-gene recurrence score of 11 to 25 (on a scale of 0 to 100, with higher scores indicating a worse prognosis or a greater potential benefit from chemotherapy) who were randomly assigned to endocrine therapy (hazard ratio for the comparison of high vs. low clinical risk, 2.73; 95% confidence interval [CI], 1.93 to 3.87) or to chemotherapy plus endocrine (chemoendocrine) therapy (hazard ratio, 2.41; 95% CI, 1.66 to 3.48) and in women with a high recurrence score (a score of 26 to 100), all of whom were assigned to chemoendocrine therapy (hazard ratio, 3.17; 95% CI, 1.94 to 5.19). Among women who were 50 years of age or younger who had received endocrine therapy alone, the estimated (±SE) rate of distant recurrence at 9 years was less than 5% (≤1.8±0.9%) with a low recurrence score (a score of 0 to 10), irrespective of clinical risk, and 4.7±1.0% with an intermediate recurrence score and low clinical risk. In this age group, the estimated distant recurrence at 9 years exceeded 10% among women with a high clinical risk and an intermediate recurrence score who received endocrine therapy alone (12.3±2.4%) and among those with a high recurrence score who received chemoendocrine therapy (15.2±3.3%).
Conclusions: Clinical-risk stratification provided prognostic information that, when added to the 21-gene recurrence score, could be used to identify premenopausal women who could benefit from more effective therapy. (Funded by the National Cancer Institute and others; ClinicalTrials.gov number, NCT00310180.).
Copyright © 2019 Massachusetts Medical Society.
Figures
Comment in
-
Clinical and Genomic Risk in Adjuvant Therapy for Breast Cancer.N Engl J Med. 2019 Sep 26;381(13):1289-1291. doi: 10.1056/NEJMc1909693. N Engl J Med. 2019. PMID: 31553844 No abstract available.
-
Clinical and Genomic Risk in Adjuvant Therapy for Breast Cancer.N Engl J Med. 2019 Sep 26;381(13):1289-1290. doi: 10.1056/NEJMc1909693. N Engl J Med. 2019. PMID: 31553845 No abstract available.
References
-
- Early Breast Cancer Trialists’ Collab-orative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005;365:1687–717. - PubMed
-
- Paik S, Shak S, Tang G, et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med 2004;351:2817–26. - PubMed
-
- Paik S, Tang G, Shak S, et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J Clin Oncol 2006;24:3726–34. - PubMed
-
- Albain KS, Barlow WE, Shak S, et al. Prognostic and predictive value of the 21-gene Recurrence Score assay in postmenopausal women with node-positive, oestrogen-receptor-positive breast cancer on chemotherapy: a retrospective analysis of a randomised trial. Lancet Oncol 2010; 11:55–65. - PMC - PubMed
-
- Sparano JA, Paik S. Development of the 21-gene assay and its application in clinical practice and clinical trials. J Clin Oncol 2008;26:721–8. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U10 CA180868/CA/NCI NIH HHS/United States
- U10 CA180801/CA/NCI NIH HHS/United States
- UG1 CA190140/CA/NCI NIH HHS/United States
- U24 CA196172/CA/NCI NIH HHS/United States
- U10 CA180795/CA/NCI NIH HHS/United States
- UG1 CA233160/CA/NCI NIH HHS/United States
- UG1 CA233373/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- U10 CA180822/CA/NCI NIH HHS/United States
- UG1 CA189804/CA/NCI NIH HHS/United States
- UG1 CA189867/CA/NCI NIH HHS/United States
- UG1 CA189859/CA/NCI NIH HHS/United States
- UG1 CA189869/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- P30 CA016086/CA/NCI NIH HHS/United States
- U10 CA180857/CA/NCI NIH HHS/United States
- U10 CA180847/CA/NCI NIH HHS/United States
- U10 CA180863/CA/NCI NIH HHS/United States
- U10 CA180790/CA/NCI NIH HHS/United States
- UG1 CA233247/CA/NCI NIH HHS/United States
- UG1 CA189808/CA/NCI NIH HHS/United States
- U10 CA180794/CA/NCI NIH HHS/United States
- UG1 CA233253/CA/NCI NIH HHS/United States
- U10 CA180799/CA/NCI NIH HHS/United States
- U10 CA180838/CA/NCI NIH HHS/United States
- U10 CA180816/CA/NCI NIH HHS/United States
- U10 CA180844/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials