

Addition of Docetaxel to First-line Long-term Hormone Therapy in Prostate Cancer (STAMPEDE): Modelling to Estimate Long-term Survival, Quality-adjusted Survival, and Cost-effectiveness
- PMID: 31158087
- PMCID: PMC6692495
- DOI: 10.1016/j.euo.2018.06.004
Addition of Docetaxel to First-line Long-term Hormone Therapy in Prostate Cancer (STAMPEDE): Modelling to Estimate Long-term Survival, Quality-adjusted Survival, and Cost-effectiveness
Abstract
Background: Results from large randomised controlled trials have shown that adding docetaxel to the standard of care (SOC) for men initiating hormone therapy for prostate cancer (PC) prolongs survival for those with metastatic disease and prolongs failure-free survival for those without. To date there has been no formal assessment of whether funding docetaxel in this setting represents an appropriate use of UK National Health Service (NHS) resources.
Objective: To assess whether administering docetaxel to men with PC starting long-term hormone therapy is cost-effective in a UK setting.
Design, setting, and participants: We modelled health outcomes and costs in the UK NHS using data collected within the STAMPEDE trial, which enrolled men with high-risk, locally advanced metastatic or recurrent PC starting first-line hormone therapy.
Intervention: SOC was hormone therapy for ≥2 yr and radiotherapy in some patients. Docetaxel (75mg/m2) was administered alongside SOC for six three-weekly cycles.
Outcome measurements and statistical analysis: The model generated lifetime predictions of costs, changes in survival duration, quality-adjusted life years (QALYs), and incremental cost-effectiveness ratios (ICERs).
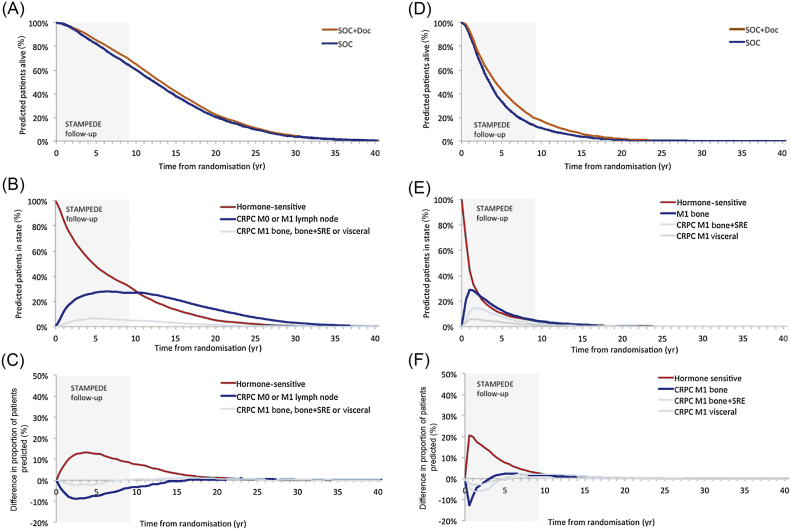
Results and limitations: The model predicted that docetaxel would extend survival (discounted quality-adjusted survival) by 0.89 yr (0.51) for metastatic PC and 0.78 yr (0.39) for nonmetastatic PC, and would be cost-effective in metastatic PC (ICER £5514/QALY vs SOC) and nonmetastatic PC (higher QALYs, lower costs vs SOC). Docetaxel remained cost-effective in nonmetastatic PC when the assumption of no survival advantage was modelled.
Conclusions: Docetaxel is cost-effective among patients with nonmetastatic and metastatic PC in a UK setting. Clinicians should consider whether the evidence is now sufficiently compelling to support docetaxel use in patients with nonmetastatic PC, as the opportunity to offer docetaxel at hormone therapy initiation will be missed for some patients by the time more mature survival data are available.
Patient summary: Starting docetaxel chemotherapy alongside hormone therapy represents a good use of UK National Health Service resources for patients with prostate cancer that is high risk or has spread to other parts of the body.
Keywords: Cost-effectiveness analysis; Docetaxel; Prostate cancer.
Copyright © 2018 The Authors. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
Building an Understanding of the Value of Docetaxel Plus Hormone Therapy in Prostate Cancer: An Ever-growing Evidence Base.Eur Urol Oncol. 2018 Dec;1(6):459-460. doi: 10.1016/j.euo.2018.10.004. Epub 2018 Nov 10. Eur Urol Oncol. 2018. PMID: 31158088 No abstract available.
References
-
- James N, Sydes M. STAMPEDE: Systemic Therapy in Advancing or Metastatic Prostate Cancer: Evaluation of Drug Efficacy, a multi-arm multi-stage randomised controlled trial. Protocol version 16. www.ctu.mrc.ac.uk/research/documents/cancer_protocols/STAMPEDE_protocol_.... - PubMed
-
- Gravis G., Boher J.M., Joly F. Androgen deprivation therapy (ADT) plus docetaxel versus ADT alone in metastatic non castrate prostate cancer: impact of metastatic burden and long-term survival analysis of the randomized phase 3 GETUG-AFU15 trial. Eur Urol. 2016;70:256–262. - PubMed
-
- Gravis G., Fizazi K., Joly F. Androgen-deprivation therapy alone or with docetaxel in non-castrate metastatic prostate cancer (GETUG-AFU 15): a randomised, open-label, phase 3 trial. Lancet Oncol. 2013;58:149–158. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
