

Factors Associated With Age Disparities Among Cancer Clinical Trial Participants
- PMID: 31158272
- PMCID: PMC6547133
- DOI: 10.1001/jamaoncol.2019.2055
Factors Associated With Age Disparities Among Cancer Clinical Trial Participants
Abstract
Importance: Seminal investigation 2 decades ago alerted the oncology community to age disparities in participation in cooperative group trials; less is known about whether these disparities persist in industry-funded research.
Objective: To characterize the age disparities among trial enrollees on randomized clinical trials (RCTs) of common cancers in clinical oncology and identify factors associated with wider age imbalances.
Data sources: Phase 3 clinical oncology RCTs were identified through ClinicalTrials.gov.
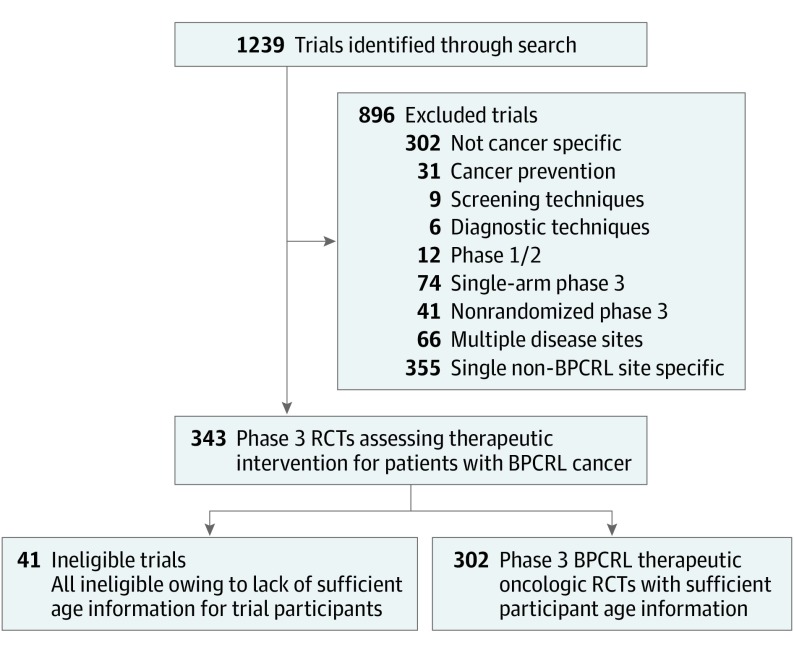
Study selection: Multiarm RCTs assessing a therapeutic intervention for patients with breast, prostate, colorectal, or lung cancer (the 4 most common cancer disease sites) were included.
Data extraction and synthesis: Trial data were extracted from ClinicalTrials.gov. Trial screening and parameter identification were independently performed by 2 individuals. Data were analyzed in 2018.
Main outcomes and measures: The difference in median age (DMA) between the trial participant median age and the population-based disease-site-specific median age was determined for each trial.
Results: Three hundred two trials met inclusion criteria. The trials collectively enrolled 262 354 participants; 249 trials (82.5%) were industry-funded. For all trials, the trial median age of trial participants was a mean of 6.49 years younger than the population median age (95% CI, -7.17 to -5.81 years; P < .001). Age disparities were heightened among industry-funded trials compared with non-industry-funded trials (mean DMA, -6.84 vs -4.72 years; P = .002). Enrollment criteria restrictions based on performance status or age cutoffs were associated with age disparities; however, industry-funded trials were not more likely to use these enrollment restrictions than non-industry-funded trials. Age disparities were also larger among trials that evaluated a targeted systemic therapy and among lung cancer trials. Linear regression modeling revealed a widening gap between trial and population median ages over time at a rate of -0.19 years annually (95% CI, -0.37 to -0.01 years; P = .04).
Conclusions and relevance: Age disparities between trial participants and the incident disease population are pervasive across trials and appear to be increasing over time. Industry sponsorship of trials is associated with heightened age imbalances among trial participants. With an increasing role of industry funding among cancer trials, efforts to understand and address age disparities are necessary to ensure generalizability of trial results as well as equity in trial access.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
