

Mid-term follow-up of staged bilateral internal carotid artery aneurysm treatment with Pipeline embolization
- PMID: 31159632
- PMCID: PMC6838859
- DOI: 10.1177/1591019919853586
Mid-term follow-up of staged bilateral internal carotid artery aneurysm treatment with Pipeline embolization
Abstract
Background: Endovascular treatment of large complex morphology aneurysms is challenging. High recanalization rates have been reported with techniques such as stent-assisted coiling and balloon-assisted coiling. Flow diverter devices have been introduced to improve efficacy outcomes and recanalization rates. Thromboembolic complications and in-device stenosis are certainly more worrisome when treatment of bilateral internal carotid arteries has been performed. This study aimed to report our experience with mid-term imaging follow-up of staged bilateral Pipeline embolization device placement for the treatment of bilateral internal carotid artery aneurysms.
Methods: We reviewed the clinical, angiographic, and follow-up imaging data in all consecutive patients treated with bilateral internal carotid artery aneurysms who underwent elective Pipeline embolization.
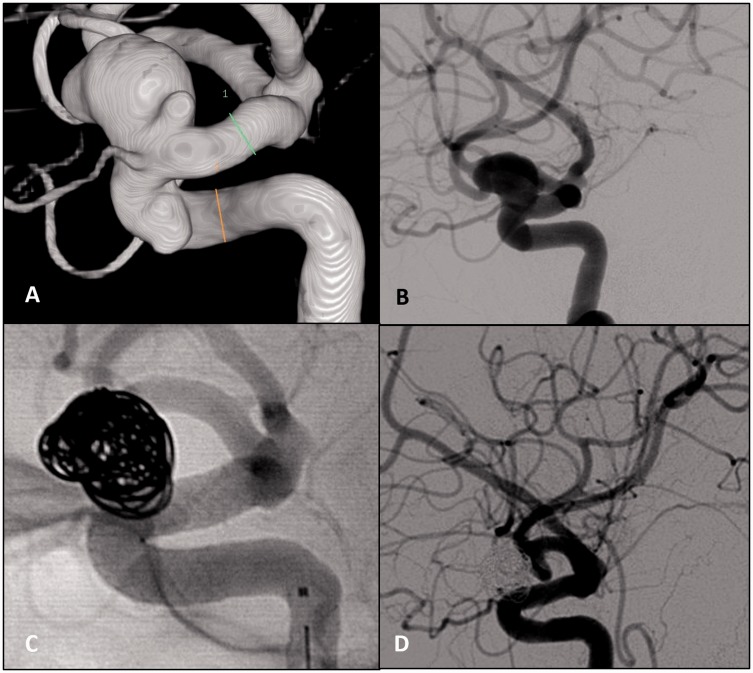
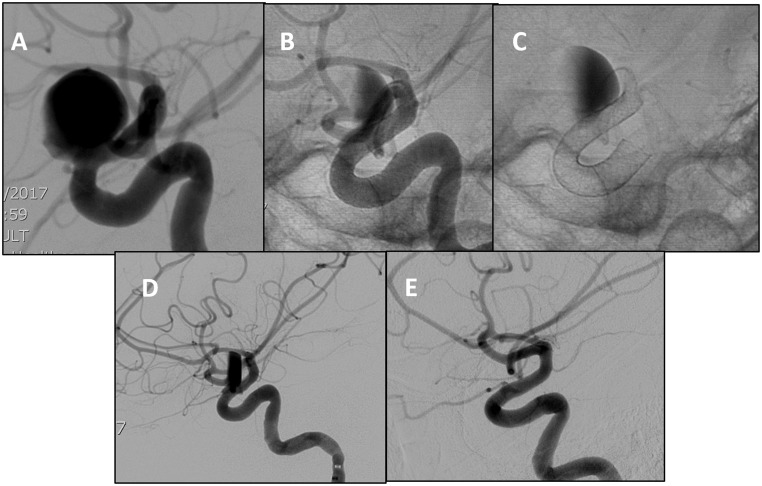
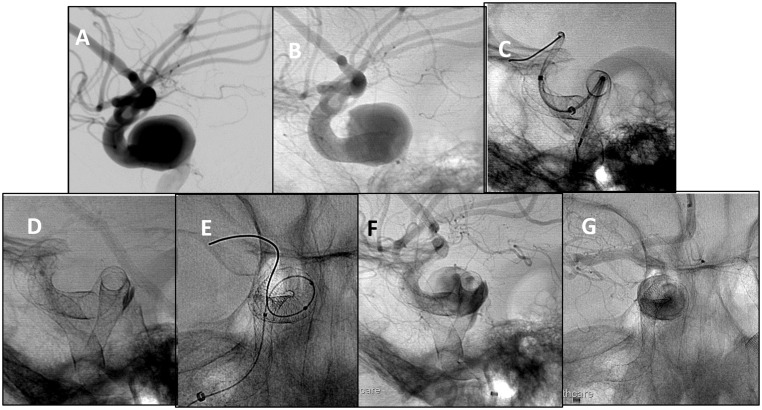
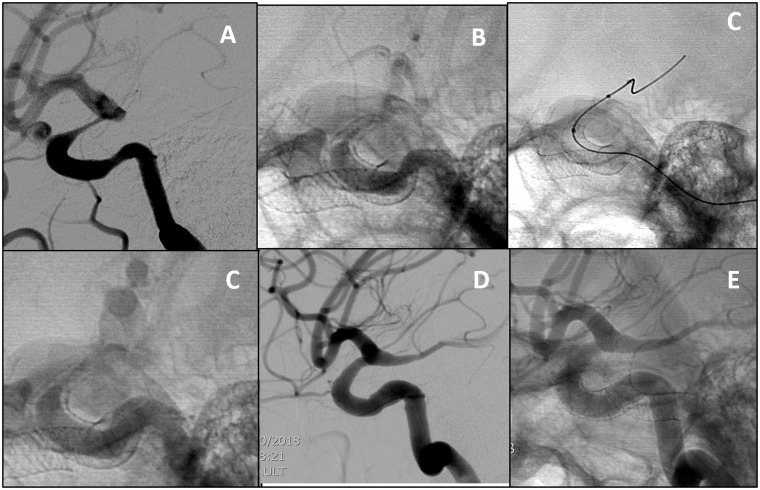
Results: Six female patients were treated, harboring a total of 13 aneurysms. Of these, 60% were asymptomatic. Diplopia and headache were the most common symptoms. The most common location was the paraclinoid segment (6/13), including by cavernous segment (4/13) and ophthalmic segment (2/13). Successful delivery of the device was achieved in 12 cases. Difficult distal access precluded the deployment of the device in one case. The treatment was always staged with at least eight weeks' difference between the two procedures. All aneurysm necks were covered completely. There were no periprocedural complications. Angiographic follow-up ranged between 3 and 12 months, and computed tomography angiogram follow-up ranged between 2 and 24 months. Complete aneurysm occlusion was achieved in all cases.
Conclusion: In our series, Pipeline deployment for the treatment of bilateral internal carotid artery aneurysms in a staged fashion is safe and feasible. Mid-term imaging follow-up showed permanent occlusion of all the treated aneurysms.
Keywords: Complex intracranial aneurysms; Pipeline embolic device; endovascular treatment; flow diverter.
Figures
References
-
- Broderick JP, Brott TG, Duldner JE, et al. Initial and recurrent bleeding are the major causes of death following subarachnoid hemorrhage. Stroke 1994; 25: 1342–1347. - PubMed
-
- Macdonald RL, Schweizer TA. Spontaneous subarachnoid haemorrhage. Lancet 2017; 389: 655–666. - PubMed
-
- Rinne J, Hernesniemi J, Puranen M, et al. Multiple intracranial aneurysms in a defined population: prospective angiographic and clinical study. Neurosurgery 1994; 35: 803–808. - PubMed
-
- Andic C, Aydemir F, Kardes O, et al. Single-stage endovascular treatment of multiple intracranial aneurysms with combined endovascular techniques: is it safe to treat all at once? J Neurointerv Surg 2017; 9: 1069–1074. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
