

Disrupted Maturation of the Microbiota and Metabolome among Extremely Preterm Infants with Postnatal Growth Failure
- PMID: 31160673
- PMCID: PMC6546715
- DOI: 10.1038/s41598-019-44547-y
Disrupted Maturation of the Microbiota and Metabolome among Extremely Preterm Infants with Postnatal Growth Failure
Abstract
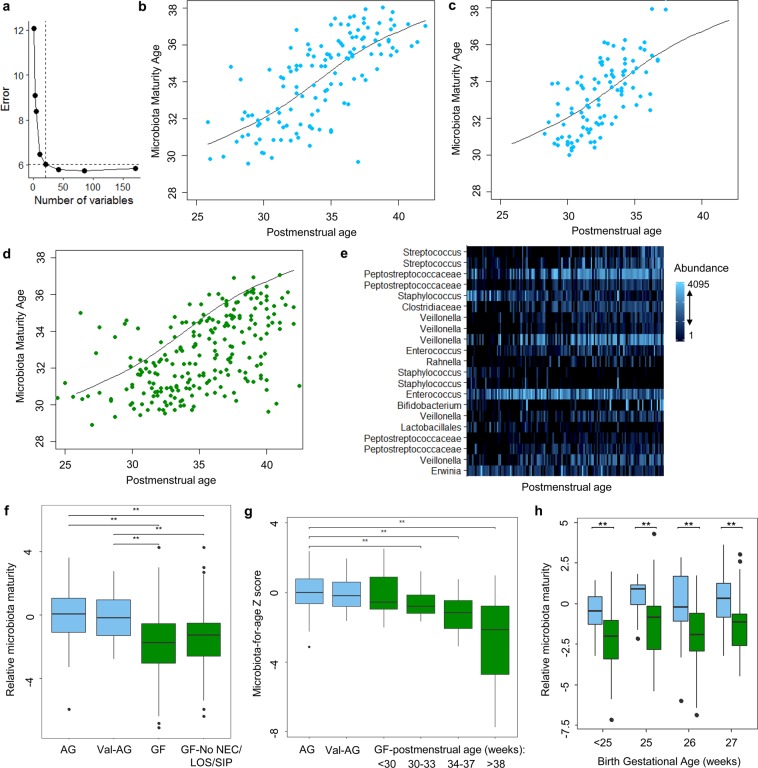
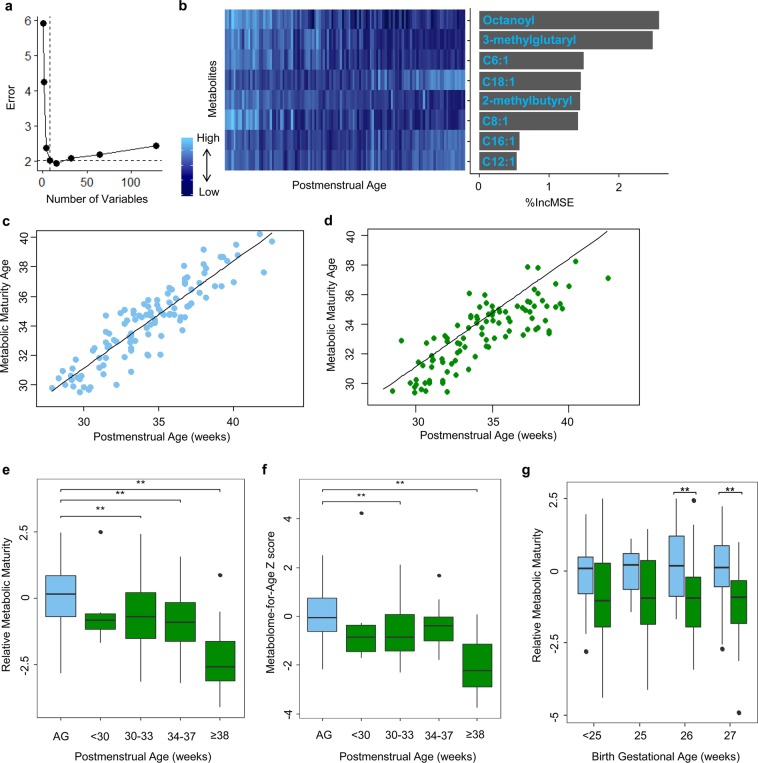
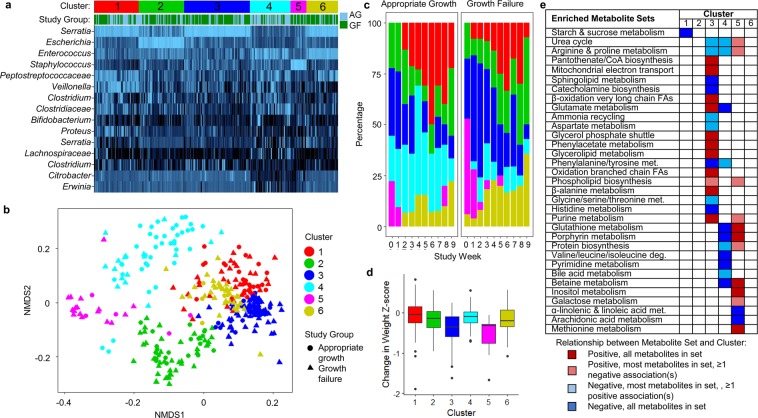
Growth failure during infancy is a major global problem that has adverse effects on long-term health and neurodevelopment. Preterm infants are disproportionately affected by growth failure and its effects. Herein we found that extremely preterm infants with postnatal growth failure have disrupted maturation of the intestinal microbiota, characterized by persistently low diversity, dominance of pathogenic bacteria within the Enterobacteriaceae family, and a paucity of strictly anaerobic taxa including Veillonella relative to infants with appropriate postnatal growth. Metabolomic profiling of infants with growth failure demonstrated elevated serum acylcarnitines, fatty acids, and other byproducts of lipolysis and fatty acid oxidation. Machine learning algorithms for normal maturation of the microbiota and metabolome among infants with appropriate growth revealed a pattern of delayed maturation of the microbiota and metabolome among infants with growth failure. Collectively, we identified novel microbial and metabolic features of growth failure in preterm infants and potentially modifiable targets for intervention.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
