

Closed-loop digital meditation improves sustained attention in young adults
- PMID: 31160812
- PMCID: PMC7534732
- DOI: 10.1038/s41562-019-0611-9
Closed-loop digital meditation improves sustained attention in young adults
Abstract
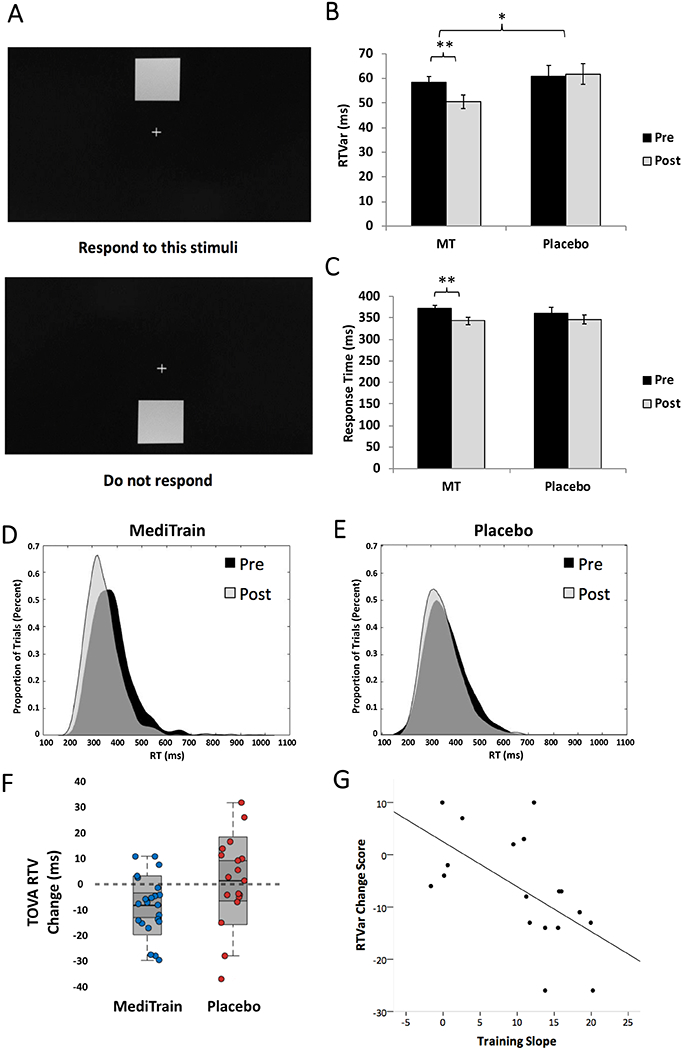
Attention is a fundamental cognitive process that is critical for essentially all aspects of higher-order cognition and real-world activities. Younger generations have deeply embraced information technology and multitasking in their personal lives, school and the workplace, creating myriad challenges to their attention. While improving sustained attention in healthy young adults would be beneficial, enhancing this ability has proven notoriously difficult in this age group. Here we show that 6 weeks of engagement with a meditation-inspired, closed-loop software program (MediTrain) delivered on mobile devices led to gains in both sustained attention and working memory in healthy young adults. These improvements were associated with positive changes in key neural signatures of attentional control (frontal theta inter-trial coherence and parietal P3b latency), as measured by electroencephalography. Our findings suggest the utility of delivering aspects of the ancient practice of focused-attention meditation in a modern, technology-based approach and its benefits on enhancing sustained attention.
Conflict of interest statement
Figures





References
-
- Rideout VJ, Foehr UG & Roberts DF Generation M2: Media in the Lives of 8- to 18-Year-Olds. (2010).
-
- Moisala M et al. Media multitasking is associated with distractibility and increased prefrontal activity in adolescents and young adults. Neuroimage 134, 113–121 (2016). - PubMed
-
- Ralph BC, Thomson DR, Cheyne JA & Smilek D Media multitasking and failures of attention in everyday life. Psychological research 78, 661–669 (2014). - PubMed
-
- Chun MM, Golomb JD & Turk-Browne NB A taxonomy of external and internal attention. Annu Rev Psychol 62, 73–101 (2011). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
