

Sepsis and septic shock: endothelial molecular pathogenesis associated with vascular microthrombotic disease
- PMID: 31160889
- PMCID: PMC6542012
- DOI: 10.1186/s12959-019-0198-4
Sepsis and septic shock: endothelial molecular pathogenesis associated with vascular microthrombotic disease
Abstract
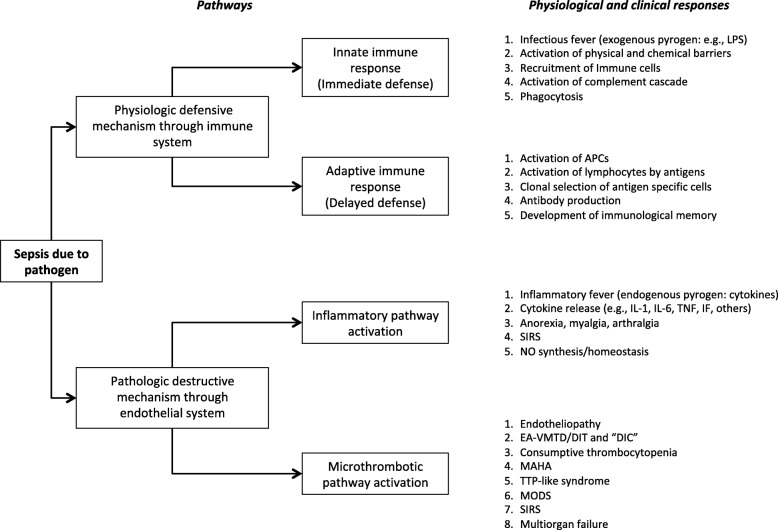
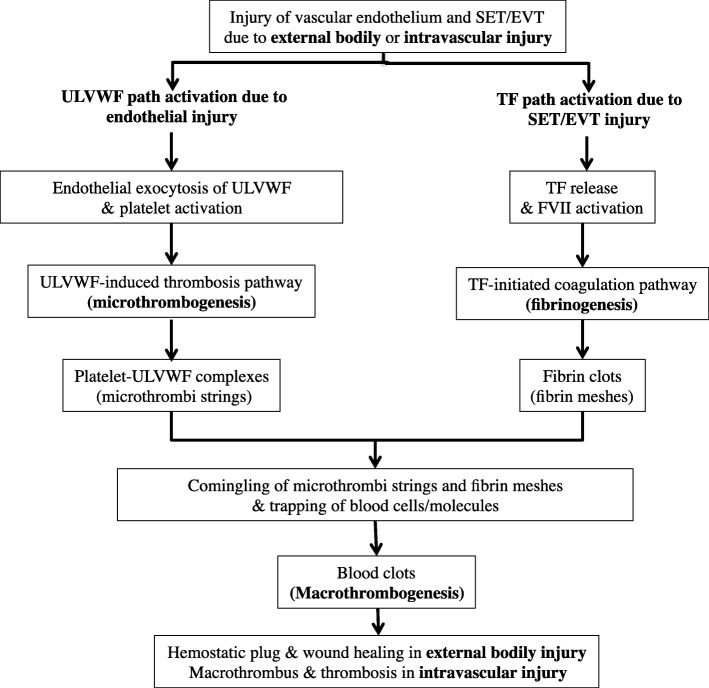
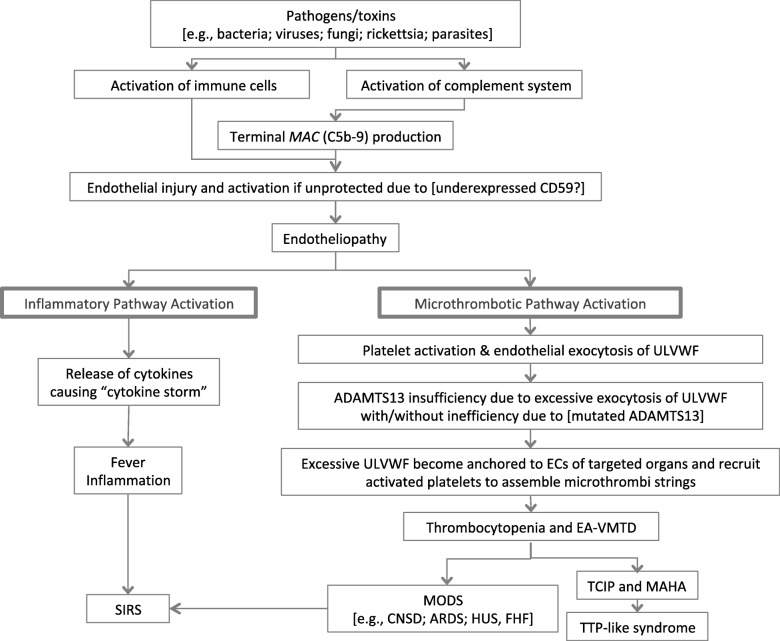
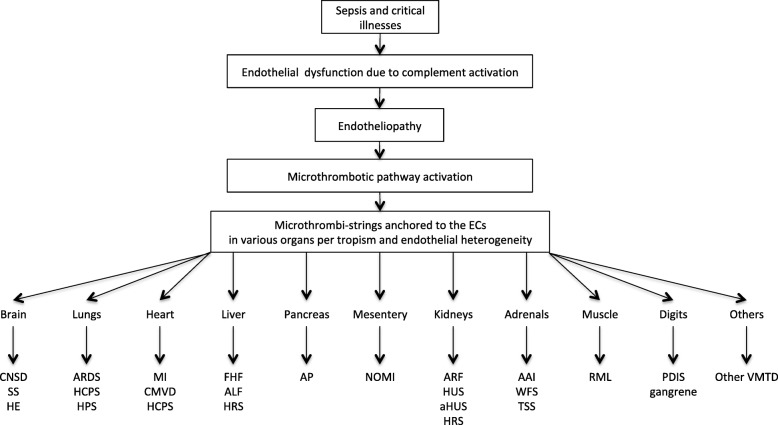
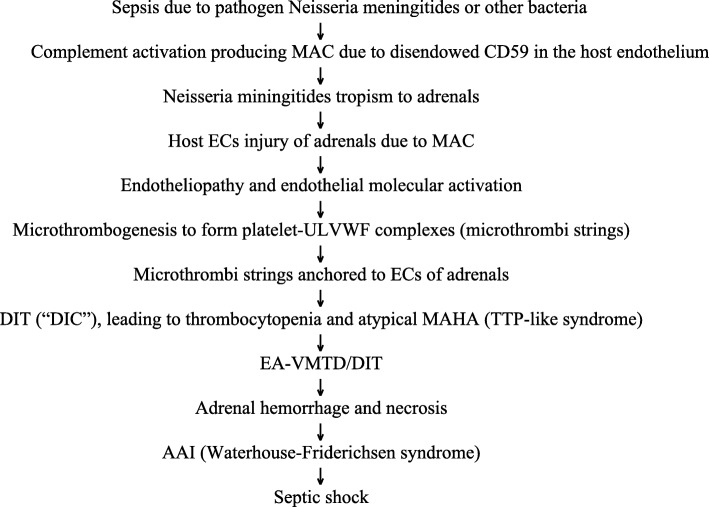
In addition to protective "immune response", sepsis is characterized by destructive "endothelial response" of the host, leading to endotheliopathy and its molecular dysfunction. Complement activation generates membrane attack complex (MAC). MAC causes channel formation to the cell membrane of pathogen, leading to death of microorganisms. In the host, MAC also may induce channel formation to innocent bystander endothelial cells (ECs) and ECs cannot be protected. This provokes endotheliopathy, which activates two independent molecular pathways: inflammatory and microthrombotic. Activated inflammatory pathway promotes the release of inflammatory cytokines and triggers inflammation. Activated microthrombotic pathway mediates platelet activation and exocytosis of unusually large von Willebrand factor multimers (ULVWF) from ECs and initiates microthrombogenesis. Excessively released ULVWF become anchored to ECs as long elongated strings and recruit activated platelets to assemble platelet-ULVWF complexes and form "microthrombi". These microthrombi strings trigger disseminated intravascular microthrombosis (DIT), which is the underlying pathology of endotheliopathy-associated vascular microthrombotic disease (EA-VMTD). Sepsis-induced endotheliopathy promotes inflammation and DIT. Inflammation produces inflammatory response and DIT orchestrates consumptive thrombocytopenia, microangiopathic hemolytic anemia, and multiorgan dysfunction syndrome (MODS). Systemic inflammatory response syndrome (SIRS) is a combined phenotype of inflammation and endotheliopathy-associated (EA)-VMTD. Successful therapeutic design for sepsis can be achieved by counteracting the pathologic microthrombogenesis.
Keywords: Anti-microthrombotic therapy; C5b-9 (membrane attack complex [MAC]); Disseminated intravascular coagulation (“DIC”, ill-founded DIC); Disseminated intravascular microthrombosis (DIT); Endotheliopathy; Microthrombogenesis; Multiorgan dysfunction syndrome (MODS); TTP-like syndrome; Therapeutic plasma exchange (TPE); Unusually large von Willebrand factor multimers (ULVWF); Vascular microthrombotic disease (VMTD).
Conflict of interest statement
Competing interestsThe author declares that he has no competing interests.
Figures

References
-
- Chang JC. Thrombocytopenia in critically ill patients due to vascular microthrombotic disease: pathogenesis based on “two activation theory of the endothelium”. Vascul Dis Ther. 2017;2:1–7. doi: 10.15761/VDT.1000132. - DOI
-
- Chang JC. Disseminated intravascular coagulation (DIC): is it fact or fancy? Blood Coagul Fibrinolysis. 2018;29:330–337. - PubMed
-
- Chang JC. Thrombogenesis and thrombotic disorders based on ‘two-path unifying theory of hemostasis’: philosophical, physiological and phenotypical interpretation. Blood Coagul Fibrinolysis. 2018;29:585–595. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
