

Exocrine Pancreatic Insufficiency Following Acute Pancreatitis: Systematic Review and Meta-Analysis
- PMID: 31161524
- PMCID: PMC6584228
- DOI: 10.1007/s10620-019-05568-9
Exocrine Pancreatic Insufficiency Following Acute Pancreatitis: Systematic Review and Meta-Analysis
Abstract
Background/objectives: The epidemiology of exocrine pancreatic insufficiency (EPI) after acute pancreatitis (AP) is uncertain. We sought to determine the prevalence, progression, etiology and pancreatic enzyme replacement therapy (PERT) requirements for EPI during follow-up of AP by systematic review and meta-analysis.
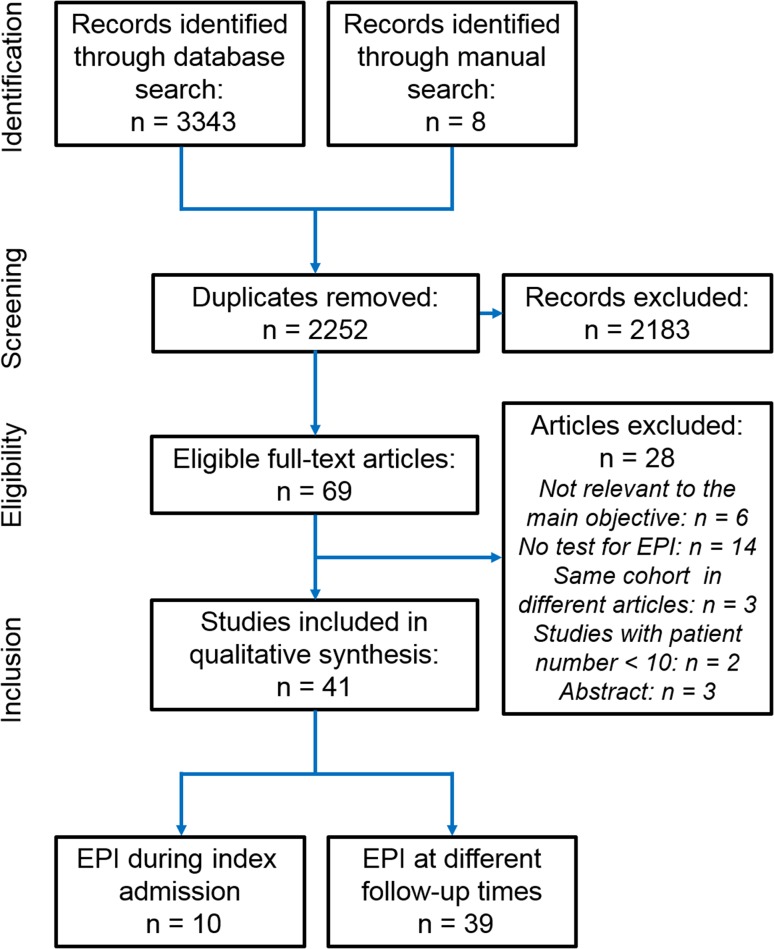
Methods: Scopus, Medline and Embase were searched for prospective observational studies or randomized clinical trials (RCTs) of PERT reporting EPI during the first admission (between the start of oral refeeding and before discharge) or follow-up (≥ 1 month of discharge) for AP in adults. EPI was diagnosed by direct and/or indirect laboratory exocrine pancreatic function tests.
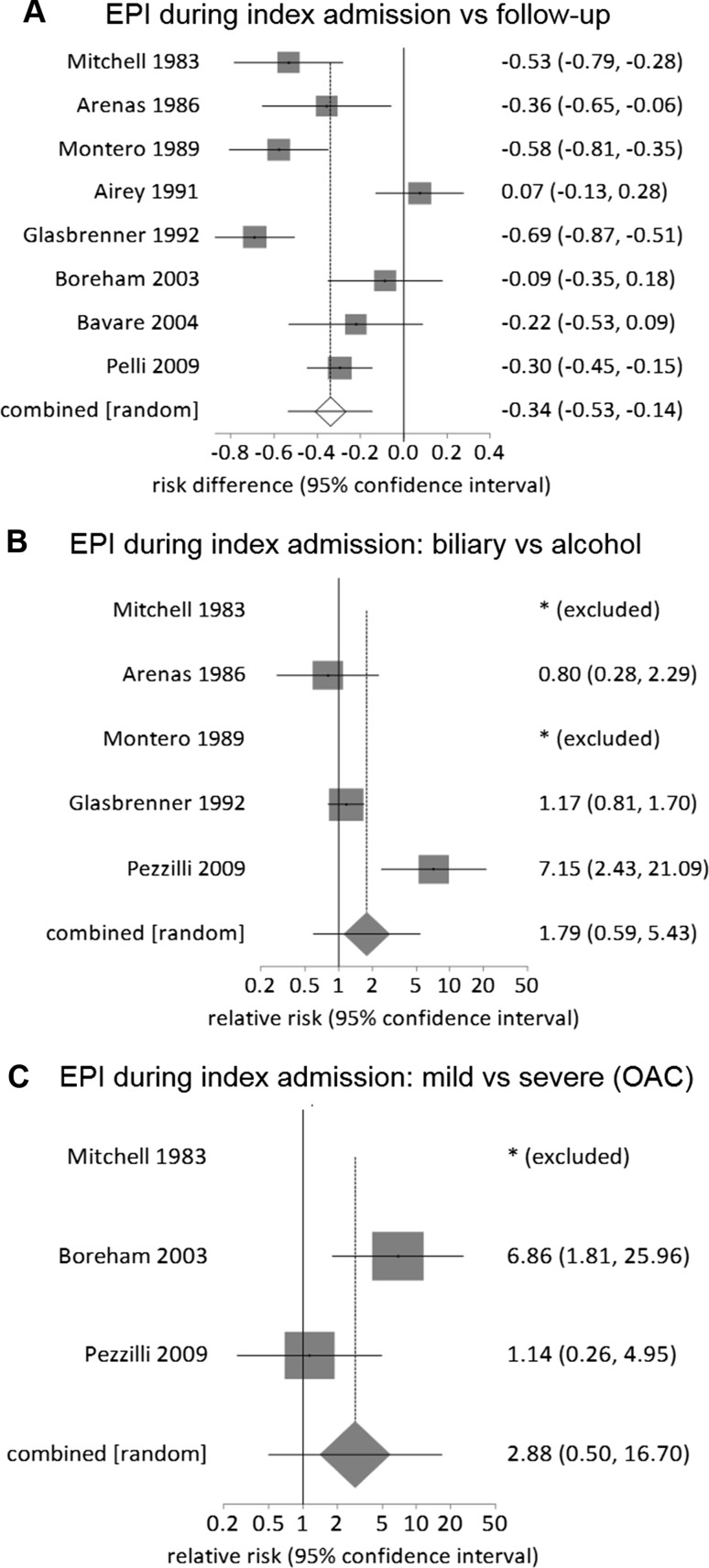
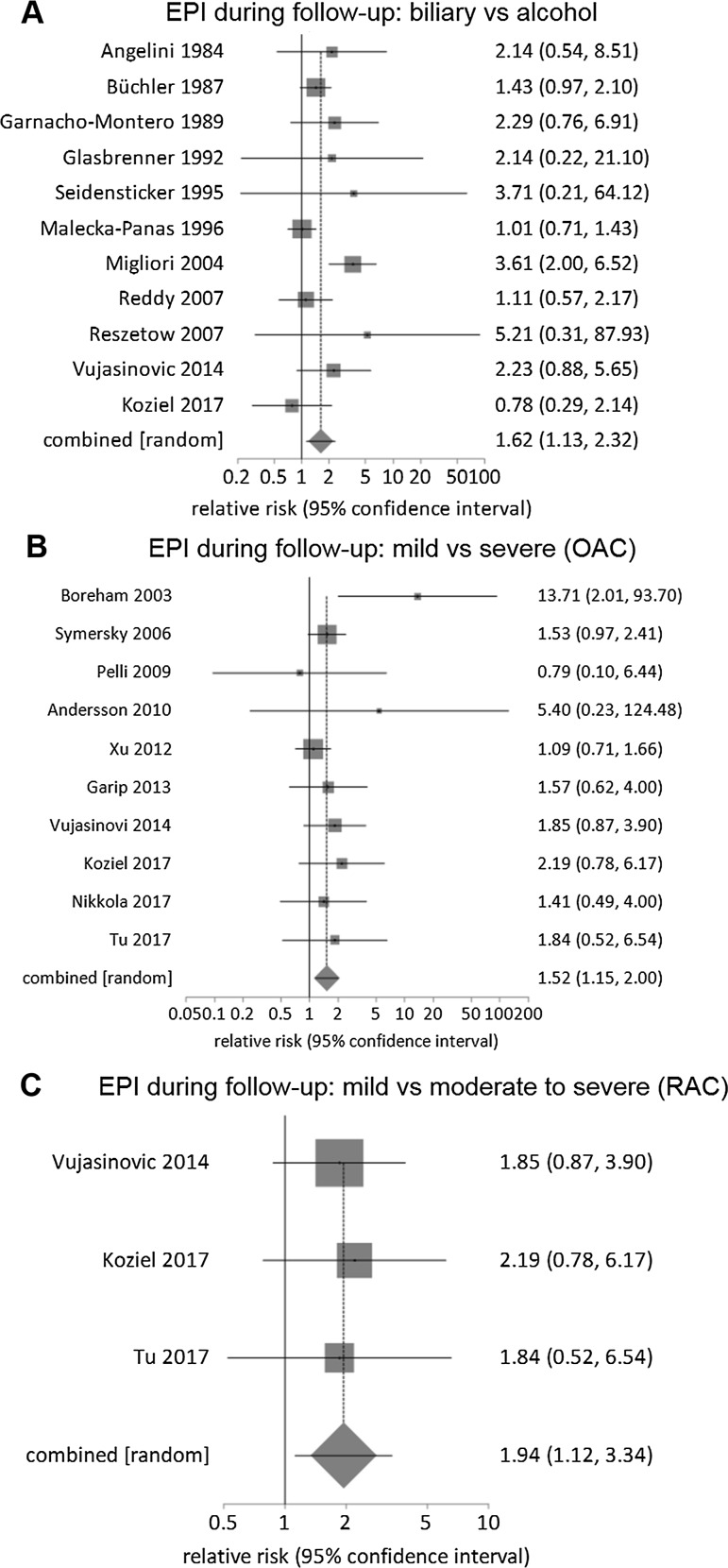
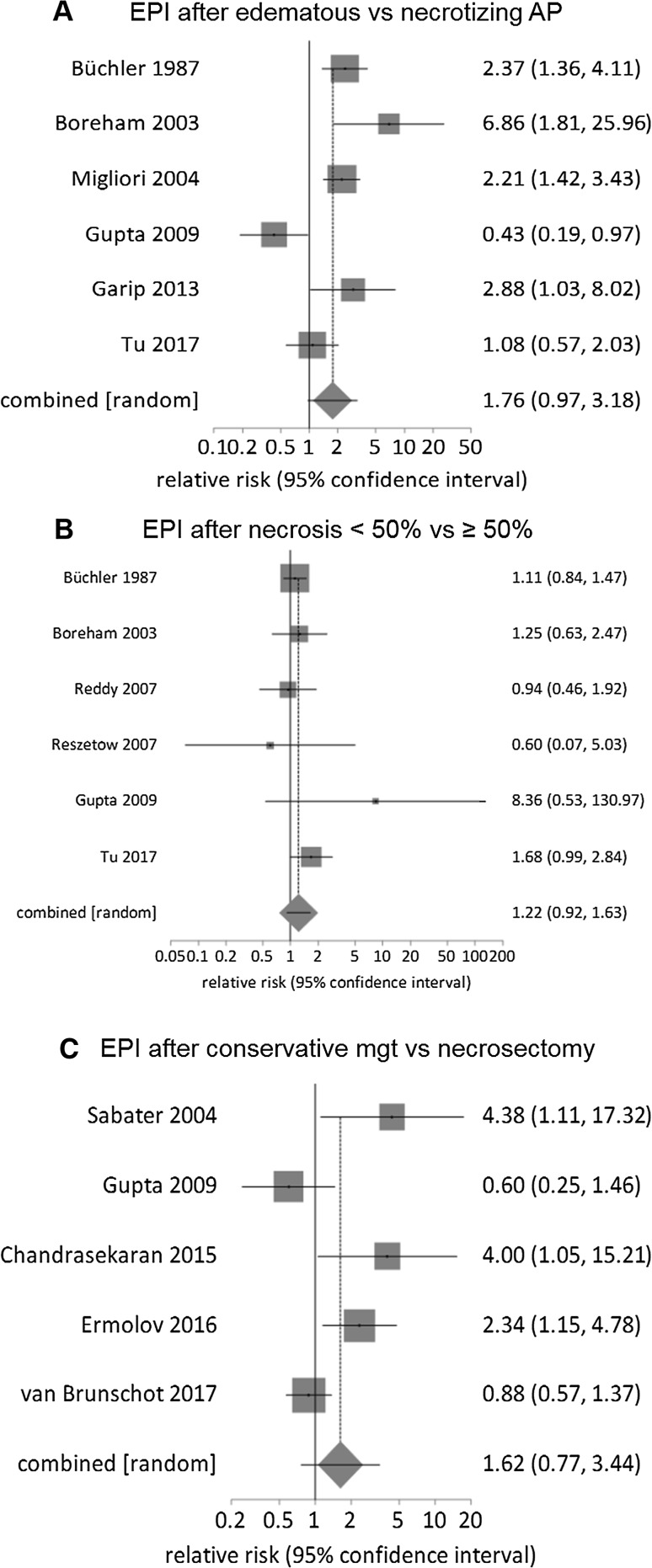
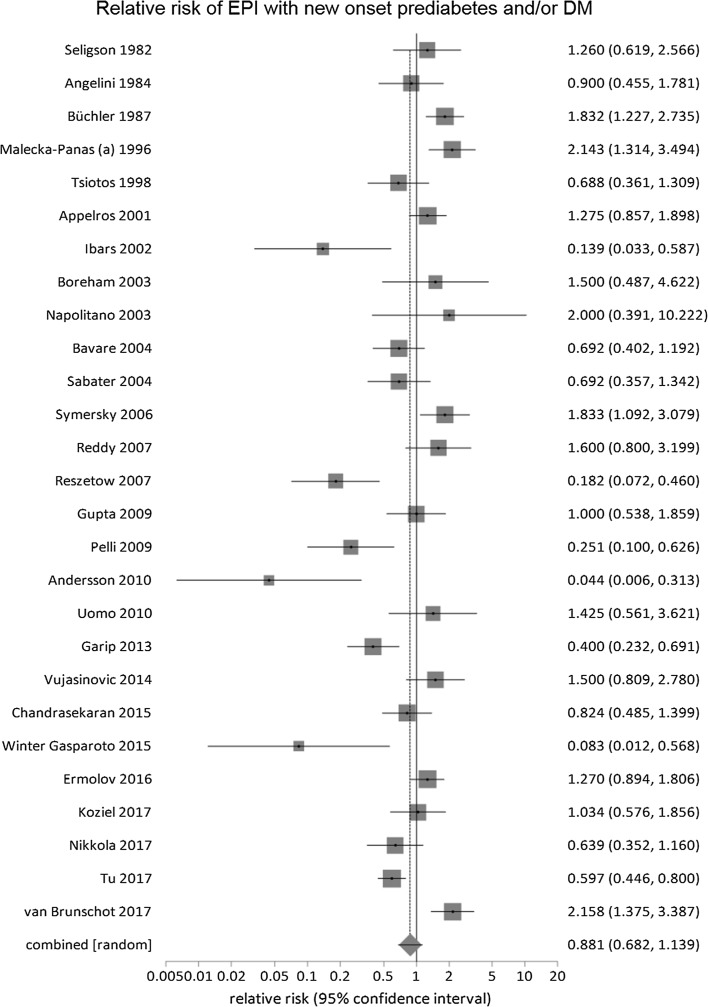
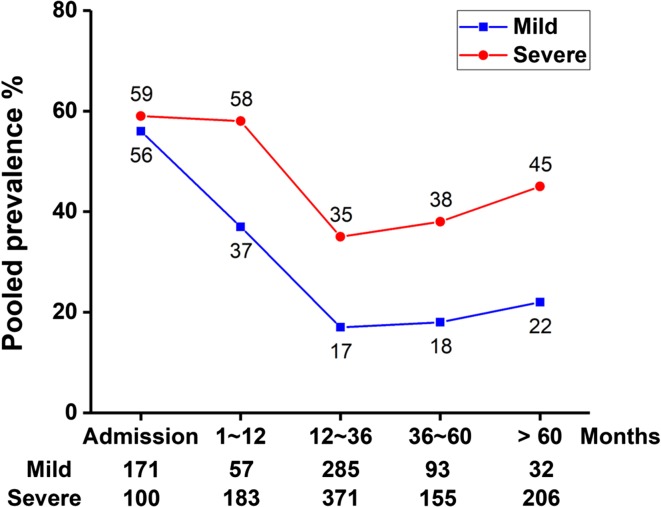
Results: Quantitative data were analyzed from 370 patients studied during admission (10 studies) and 1795 patients during follow-up (39 studies). The pooled prevalence of EPI during admission was 62% (95% confidence interval: 39-82%), decreasing significantly during follow-up to 35% (27-43%; risk difference: - 0.34, - 0.53 to - 0.14). There was a two-fold increase in the prevalence of EPI with severe compared with mild AP, and it was higher in patients with pancreatic necrosis and those with an alcohol etiology. The prevalence decreased during recovery, but persisted in a third of patients. There was no statistically significant difference between EPI and new-onset pre-diabetes/diabetes (risk difference: 0.8, 0.7-1.1, P = 0.33) in studies reporting both. Sensitivity analysis showed fecal elastase-1 assay detected significantly fewer patients with EPI than other tests.
Conclusions: The prevalence of EPI during admission and follow-up is substantial in patients with a first attack of AP. Unanswered questions remain about the way this is managed, and further RCTs are indicated.
Keywords: Acute pancreatitis; Exocrine pancreatic insufficiency; Necrotizing pancreatitis; Pancreatic enzyme replacement therapy; Severe pancreatitis.
Conflict of interest statement
JED-M has provided consultancy to and received financial support from Abbott (Mylan) for lecture fees and travel expenses outside of the submitted work; RS has provided consultancy to Abbott (Mylan); no further support from any organization for the submitted work; no the financial relationships with any organizations that might have had an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Exocrine Pancreatic Insufficiency Following Acute Pancreatitis: True Association or EPIphenomenon?Dig Dis Sci. 2019 Jul;64(7):1731-1733. doi: 10.1007/s10620-019-05653-z. Dig Dis Sci. 2019. PMID: 31076987 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
