

Understanding and Enhancing Sepsis Survivorship. Priorities for Research and Practice
- PMID: 31161771
- PMCID: PMC6794113
- DOI: 10.1164/rccm.201812-2383CP
Understanding and Enhancing Sepsis Survivorship. Priorities for Research and Practice
Abstract
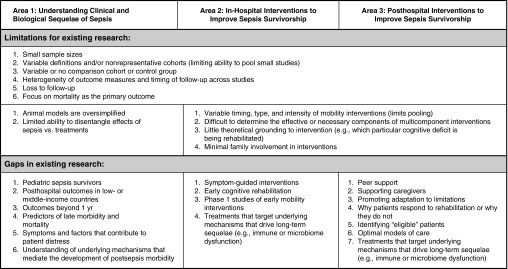
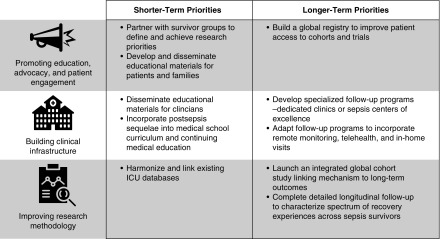
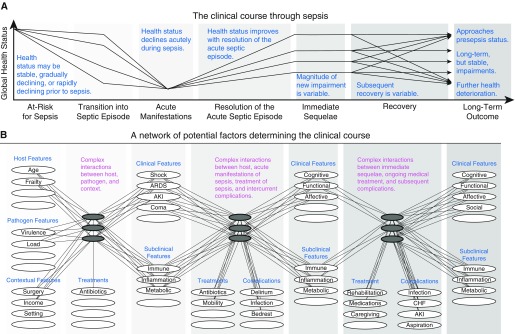
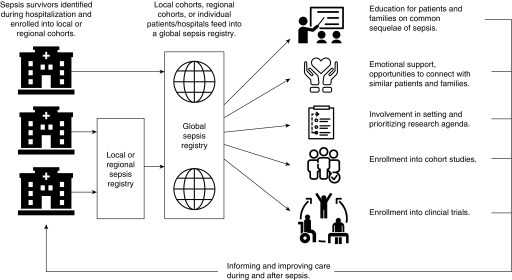
An estimated 14.1 million patients survive sepsis each year. Many survivors experience poor long-term outcomes, including new or worsened neuropsychological impairment; physical disability; and vulnerability to further health deterioration, including recurrent infection, cardiovascular events, and acute renal failure. However, clinical trials and guidelines have focused on shorter-term survival, so there are few data on promoting longer-term recovery. To address this unmet need, the International Sepsis Forum convened a colloquium in February 2018 titled "Understanding and Enhancing Sepsis Survivorship." The goals were to identify gaps and limitations of current research and shorter- and longer-term priorities for understanding and enhancing sepsis survivorship. Twenty-six experts from eight countries participated. The top short-term priorities identified by nominal group technique culminating in formal voting were to better leverage existing databases for research, develop and disseminate educational resources on postsepsis morbidity, and partner with sepsis survivors to define and achieve research priorities. The top longer-term priorities were to study mechanisms of long-term morbidity through large cohort studies with deep phenotyping, build a harmonized global sepsis registry to facilitate enrollment in cohorts and trials, and complete detailed longitudinal follow-up to characterize the diversity of recovery experiences. This perspective reviews colloquium discussions, the identified priorities, and current initiatives to address them.
Keywords: critical illness; rehabilitation; survivorship.
Figures
References
-
- Fleischmann C, Scherag A, Adhikari NKJ, Hartog CS, Tsaganos T, Schlattmann P, et al. International Forum of Acute Care Trialists. Assessment of global incidence and mortality of hospital-treated sepsis: current estimates and limitations. Am J Respir Crit Care Med. 2016;193:259–272. - PubMed
-
- Fleischmann-Struzek C, Goldfarb DM, Schlattmann P, Schlapbach LJ, Reinhart K, Kissoon N. The global burden of paediatric and neonatal sepsis: a systematic review. Lancet Respir Med. 2018;6:223–230. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
