

Intracranial Hypertension and Cerebral Perfusion Pressure Insults in Adult Hypertensive Intraventricular Hemorrhage: Occurrence and Associations With Outcome
- PMID: 31162192
- PMCID: PMC7490004
- DOI: 10.1097/CCM.0000000000003848
Intracranial Hypertension and Cerebral Perfusion Pressure Insults in Adult Hypertensive Intraventricular Hemorrhage: Occurrence and Associations With Outcome
Abstract
Objectives: Elevated intracranial pressure and inadequate cerebral perfusion pressure may contribute to poor outcomes in hypertensive intraventricular hemorrhage. We characterized the occurrence of elevated intracranial pressure and low cerebral perfusion pressure in obstructive intraventricular hemorrhage requiring extraventricular drainage.
Design: Prospective observational cohort.
Setting: ICUs of 73 academic hospitals.
Patients: Four hundred ninety-nine patients enrolled in the CLEAR III trial, a multicenter, randomized study to determine if extraventricular drainage plus intraventricular alteplase improved outcome versus extraventricular drainage plus saline.
Interventions: Intracranial pressure and cerebral perfusion pressure were recorded every 4 hours, analyzed over a range of thresholds, as single readings or spans (≥ 2) of readings after adjustment for intracerebral hemorrhage severity. Impact on 30- and 180-days modified Rankin Scale scores was assessed, and receiver operating curves were analyzed to identify optimal thresholds.
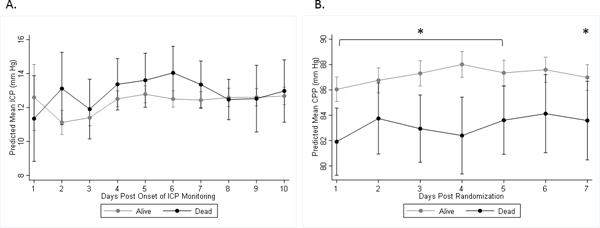
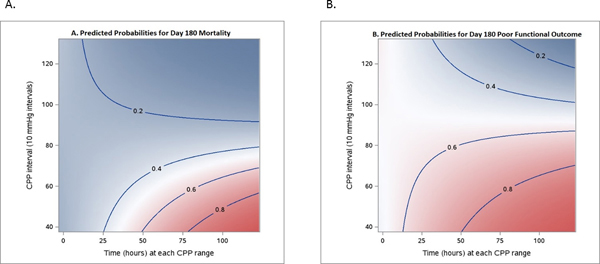
Measurements and main results: Of 21,954 intracranial pressure readings, median interquartile range 12 mm Hg (8-16), 9.7% were greater than 20 mm Hg and 1.8% were greater than 30 mm Hg. Proportion of intracranial pressure readings from greater than 18 to greater than 30 mm Hg and combined intracranial pressure greater than 20 plus cerebral perfusion pressure less than 70 mm Hg were associated with day-30 mortality and partially mitigated by intraventricular alteplase. Proportion of cerebral perfusion pressure readings from less than 65 to less than 90 mm Hg and intracranial pressure greater than 20 mm Hg in spans were associated with both 30-day mortality and 180-day mortality. Proportion of cerebral perfusion pressure readings from less than 65 to less than 90 mm Hg and combined intracranial pressure greater than 20 plus cerebral perfusion pressure less than 60 mm Hg were associated with poor day-30 modified Rankin Scale, whereas cerebral perfusion pressure less than 65 and less than 75 mm Hg were associated with poor day-180 modified Rankin Scale.
Conclusions: Elevated intracranial pressure and inadequate cerebral perfusion pressure are not infrequent during extraventricular drainage for severe intraventricular hemorrhage, and level and duration predict higher short-term mortality and long-term mortality. Burden of low cerebral perfusion pressure was also associated with poor short- and long-term outcomes and may be more significant than intracranial pressure. Adverse consequences of intracranial pressure-time burden and cerebral perfusion pressure-time burden should be tested prospectively as potential thresholds for therapeutic intervention.
Figures
References
-
- Hemphill JC 3rd, Greenberg SM, Anderson CS, et al.: Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2015; 46:2032–2060 - PubMed
-
- Ropper AH, King RB: Intracranial pressure monitoring in comatose patients with cerebral hemorrhage. Arch Neurol 1984; 41:725–728 - PubMed
-
- Janny P, Papo I, Chazal J, et al.: Intracranial hypertension and prognosis of spontaneous intracerebral haematomas. A correlative study of 60 patients. Acta Neurochir (Wien) 1982; 61:181–186 - PubMed
-
- Fernandes HM, Siddique S, Banister K, et al.: Continuous monitoring of ICP and CPP following ICH and its relationship to clinical, radiological and surgical parameters. Acta Neurochir Suppl 2000; 76:463–466 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
