

Impact of Telemonitoring of Critically Ill Emergency Department Patients Awaiting ICU Transfer
- PMID: 31162198
- PMCID: PMC8600975
- DOI: 10.1097/CCM.0000000000003847
Impact of Telemonitoring of Critically Ill Emergency Department Patients Awaiting ICU Transfer
Abstract
Objectives: Because of overcrowding and limited critical care resources, critically ill patients in the emergency department may spend hours to days awaiting transfer to the ICU. In these patients, often termed "ICU boarders," delayed ICU transfer is associated with poor outcomes. We implemented an emergency department-based, electronic ICU monitoring system for ICU boarders. Our aim was to investigate the effect of this initiative on morbidity, mortality, and ICU usage.
Design: Single-center, retrospective cohort study.
Setting: Nonprofit, tertiary care, teaching hospital with greater than 100,000 emergency department visits per year.
Patients: Emergency department patients with admission orders for the medical ICU, who spent more than 2 hours boarding in the emergency department after being accepted for admission to the medical ICU, were included in the study.
Interventions: None.
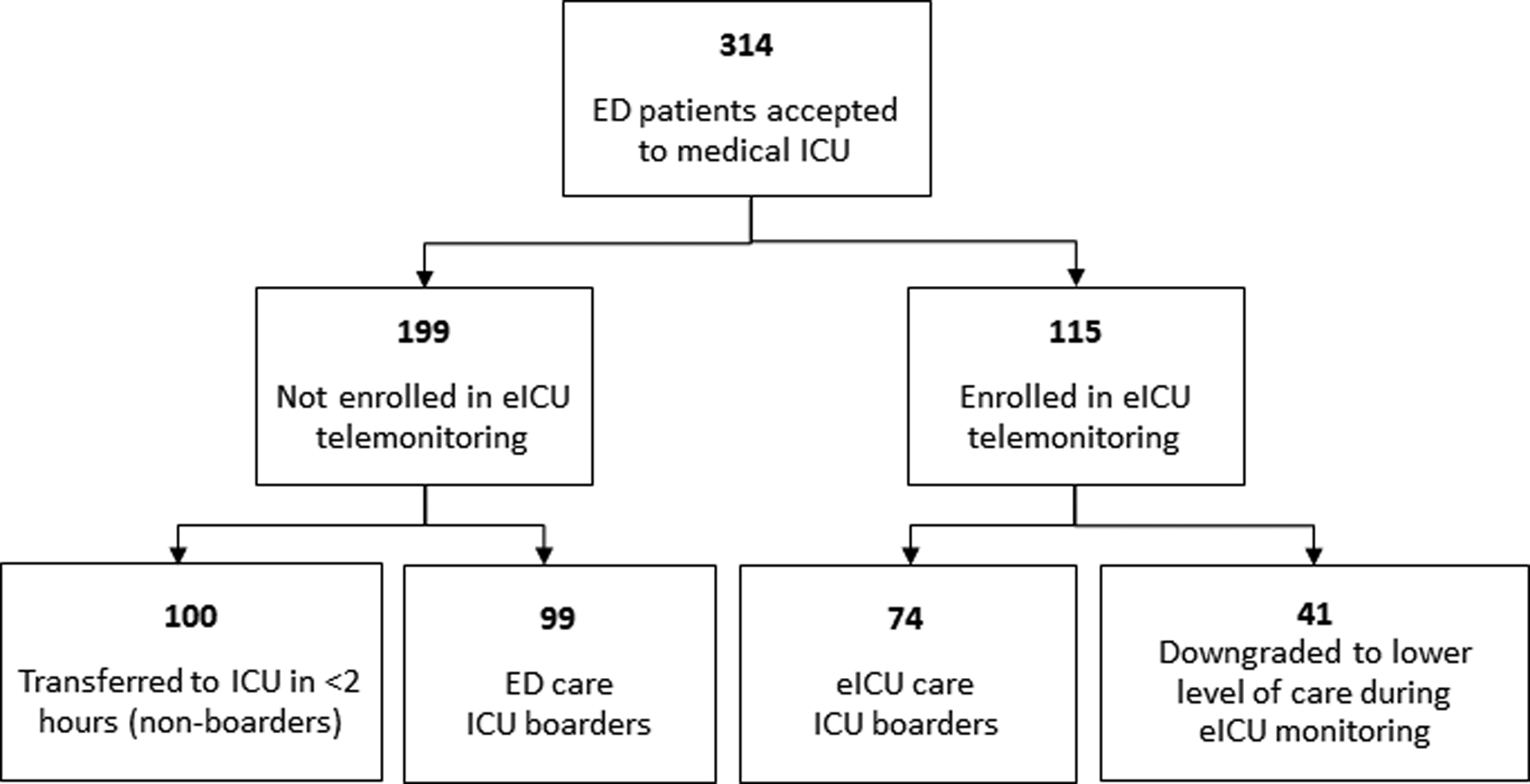
Measurements and main results: During the study period, a total of 314 patients were admitted to the medical ICU from the emergency department, 214 of whom were considered ICU boarders with a delay in medical ICU transfer over 2 hours. Of ICU boarders, 115 (53.7%) were enrolled in electronic ICU telemonitoring (electronic ICU care), and the rest received usual emergency department care (emergency department care). Age, mean illness severity (Acute Physiology and Chronic Health Evaluation IVa scores), and admitting diagnoses did not differ significantly between ICU boarders receiving electronic ICU care and emergency department care. Forty-one electronic ICU care patients (36%) were ultimately transitioned to a less intensive level of care in lieu of ICU admission while still in the emergency department, compared with zero patients in the emergency department care group. Among all ICU boarders transferred to the ICU, in-hospital mortality was lower in the electronic ICU care cohort when compared with the emergency department care cohort (5.4% vs 20.0%; adjusted odds ratio, 0.08).
Conclusions: In critically ill patients awaiting transfer from the emergency department to the medical ICU, electronic ICU care was associated with decreased mortality and lower ICU resource utilization.
Figures
Comment in
-
Critical Care Surge Management: A Role for ICU Telemedicine and Emergency Department Collaboration.Crit Care Med. 2019 Sep;47(9):1271-1273. doi: 10.1097/CCM.0000000000003881. Crit Care Med. 2019. PMID: 31415312 No abstract available.
References
-
- Mullins PM, Goyal M, Pines JM: National growth in intensive care unit admissions from emergency departments in the United States from 2002 to 2009. Acad Emerg Med 2013, 20(5):479–486. - PubMed
-
- Halpern NA, Pastores SM: Critical care medicine in the United States 2000–2005: an analysis of bed numbers, occupancy rates, payer mix, and costs. Crit Care Med 2010, 38(1):65–71. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
