

Single-cell transcriptome analyses reveal novel targets modulating cardiac neovascularization by resident endothelial cells following myocardial infarction
- PMID: 31162546
- PMCID: PMC6685329
- DOI: 10.1093/eurheartj/ehz305
Single-cell transcriptome analyses reveal novel targets modulating cardiac neovascularization by resident endothelial cells following myocardial infarction
Abstract
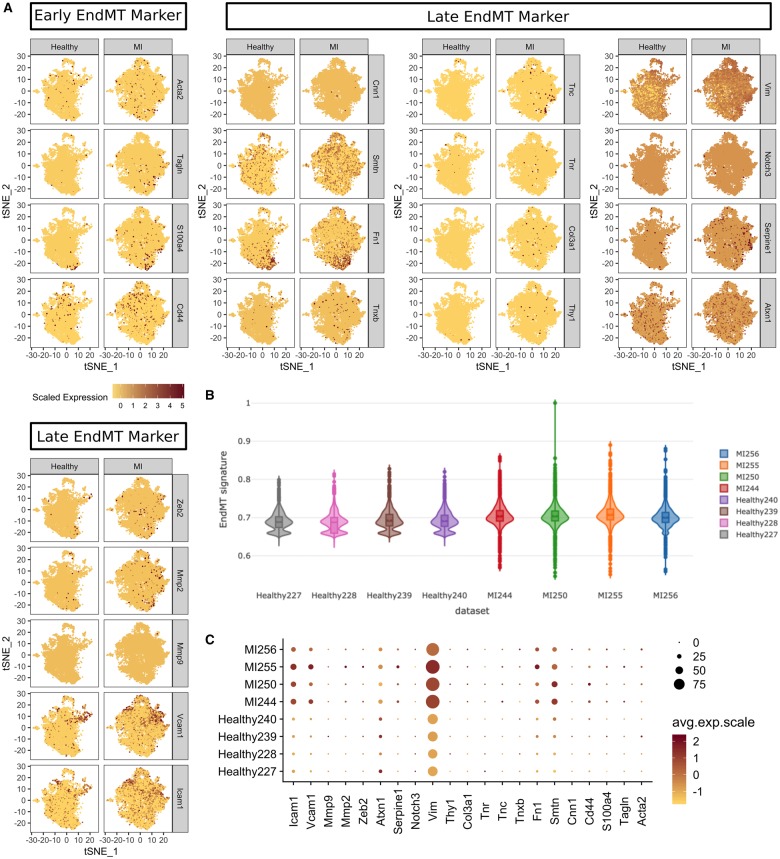
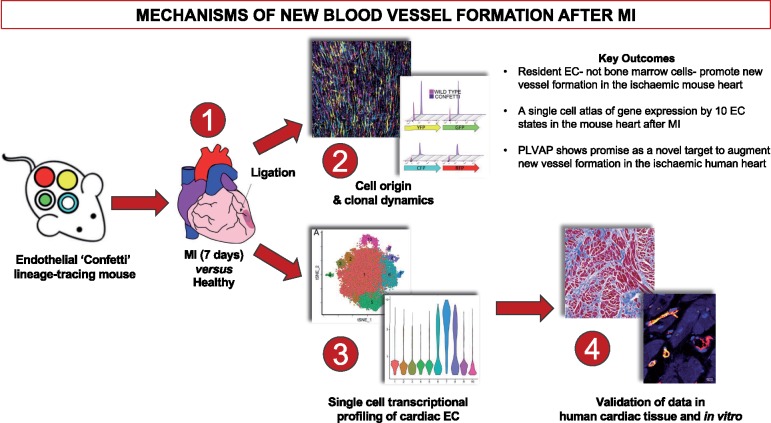
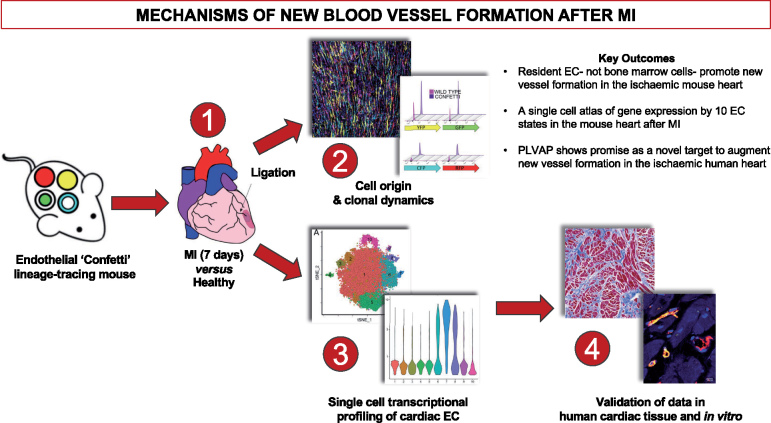
Aims: A better understanding of the pathways that regulate regeneration of the coronary vasculature is of fundamental importance for the advancement of strategies to treat patients with heart disease. Here, we aimed to investigate the origin and clonal dynamics of endothelial cells (ECs) associated with neovascularization in the adult mouse heart following myocardial infarction (MI). Furthermore, we sought to define murine cardiac endothelial heterogeneity and to characterize the transcriptional profiles of pro-angiogenic resident ECs in the adult mouse heart, at single-cell resolution.
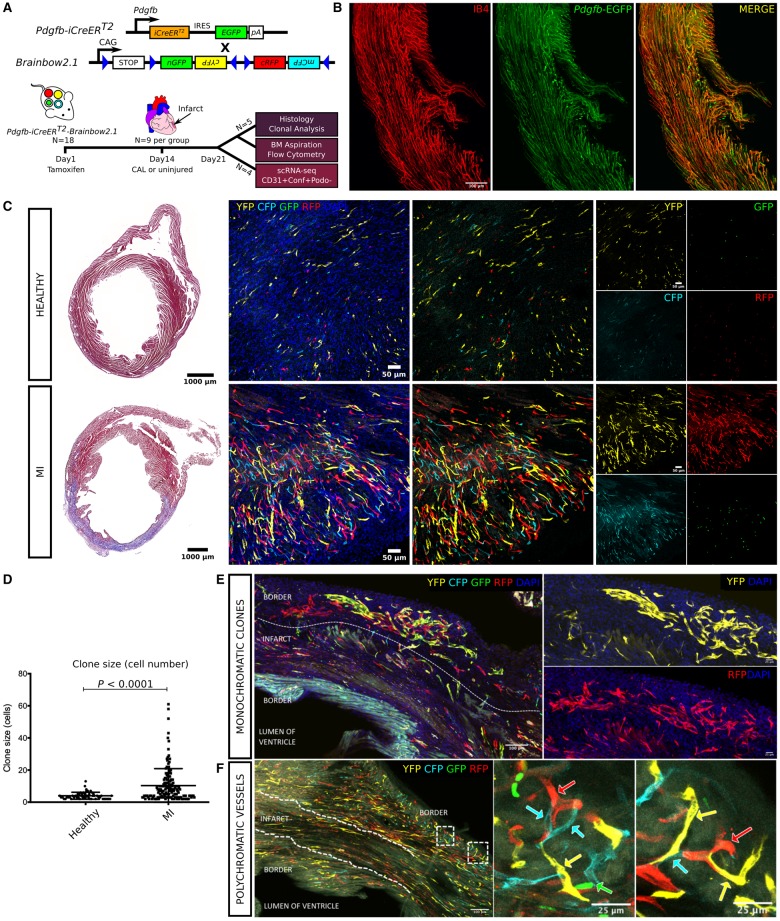
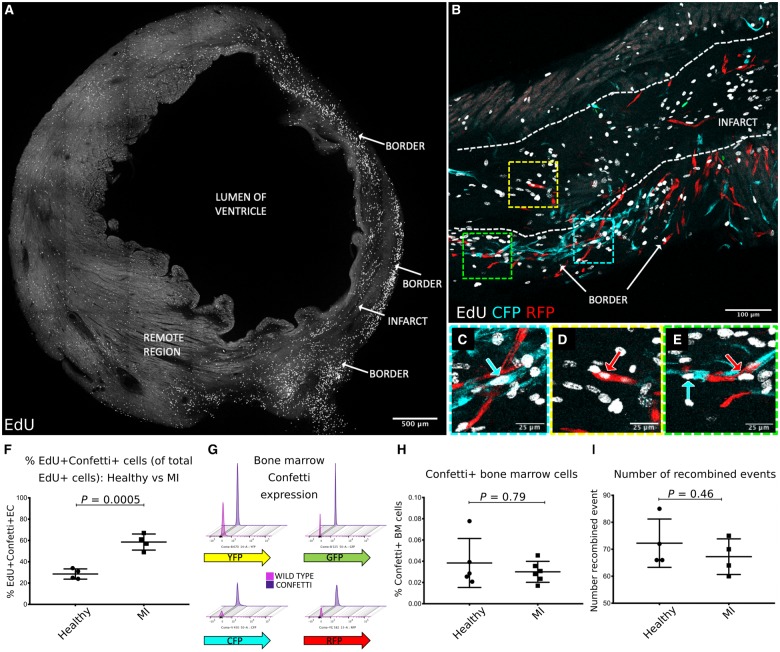
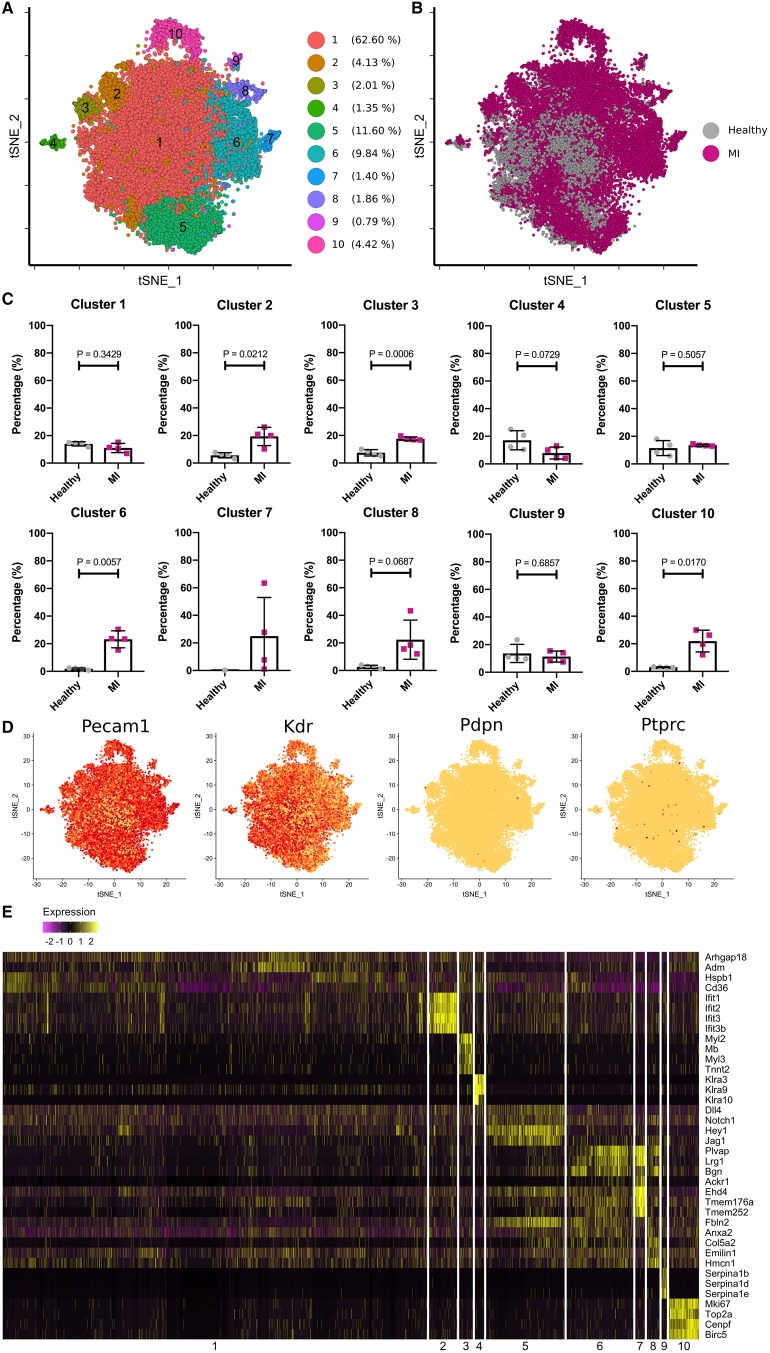
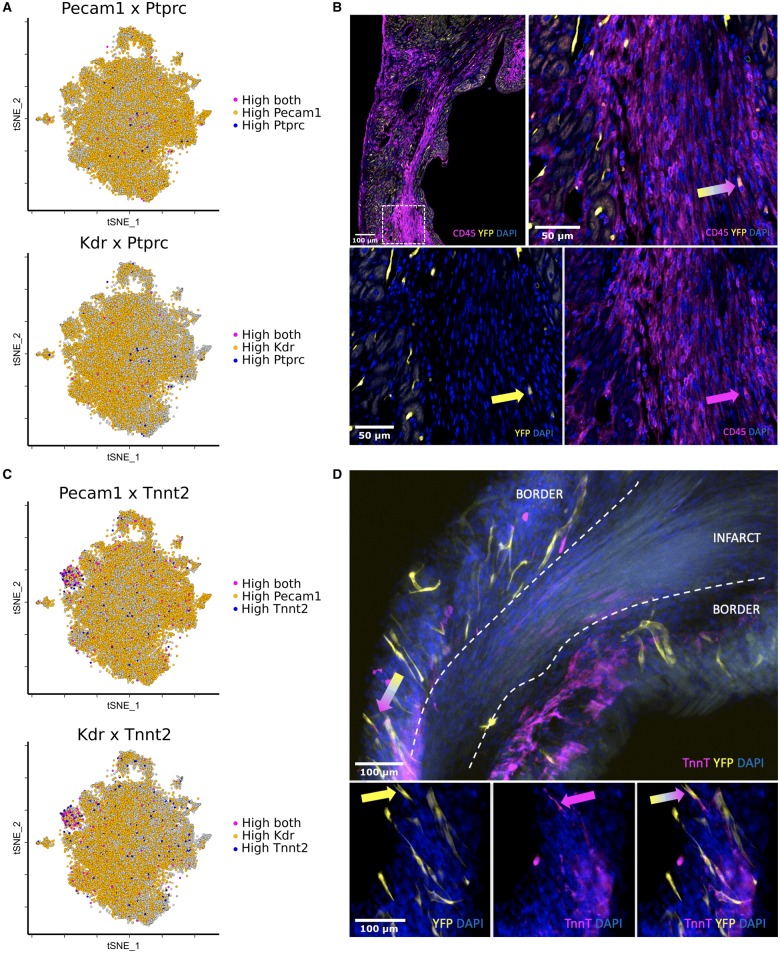
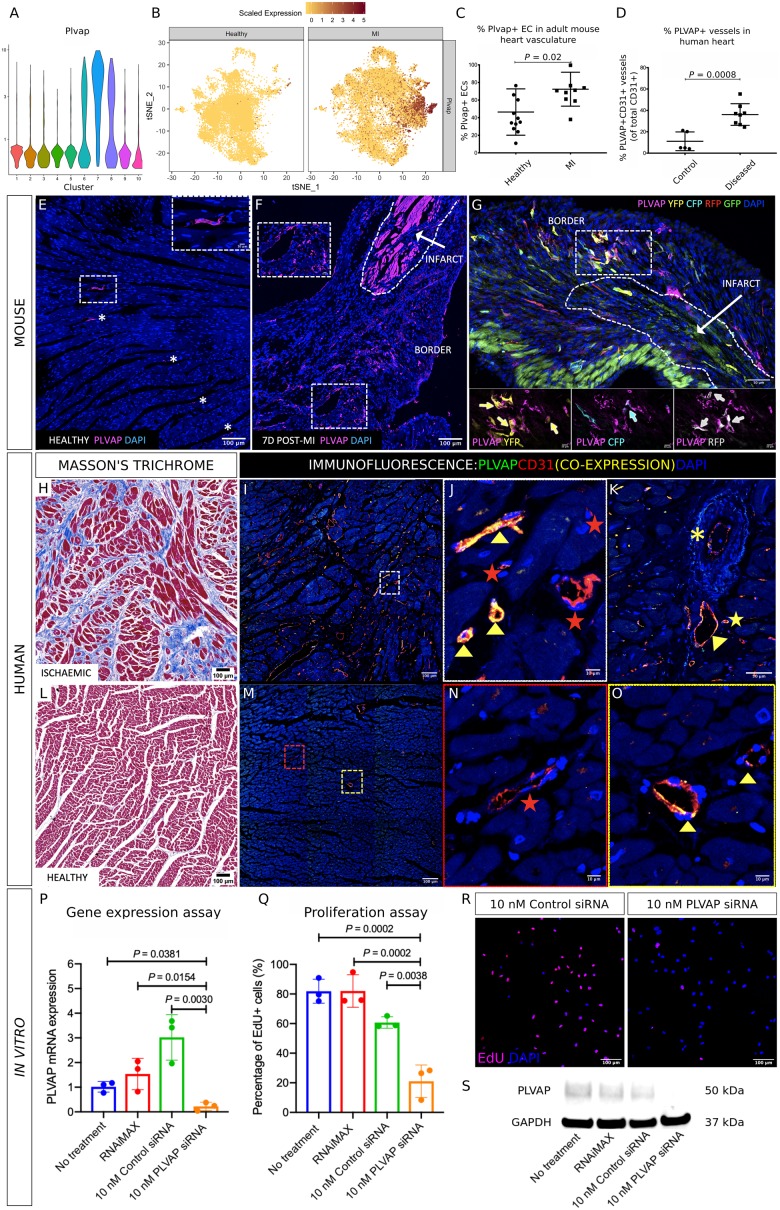
Methods and results: An EC-specific multispectral lineage-tracing mouse (Pdgfb-iCreERT2-R26R-Brainbow2.1) was used to demonstrate that structural integrity of adult cardiac endothelium following MI was maintained through clonal proliferation by resident ECs in the infarct border region, without significant contributions from bone marrow cells or endothelial-to-mesenchymal transition. Ten transcriptionally discrete heterogeneous EC states, as well as the pathways through which each endothelial state is likely to enhance neovasculogenesis and tissue regeneration following ischaemic injury were defined. Plasmalemma vesicle-associated protein (Plvap) was selected for further study, which showed an endothelial-specific and increased expression in both the ischaemic mouse and human heart, and played a direct role in regulating human endothelial proliferation in vitro.
Conclusion: We present a single-cell gene expression atlas of cardiac specific resident ECs, and the transcriptional hierarchy underpinning endogenous vascular repair following MI. These data provide a rich resource that could assist in the development of new therapeutic interventions to augment endogenous myocardial perfusion and enhance regeneration in the injured heart.
Keywords: Cell proliferation; Endothelial cells; Lineage tracing; Myocardial infarction; Single-cell RNA sequencing; Therapeutic angiogenesis.
© The Author(s) 2019. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Clonal and diverse: revisiting cardiac endothelial cells after myocardial infarction.Eur Heart J. 2019 Aug 7;40(30):2521-2522. doi: 10.1093/eurheartj/ehz375. Eur Heart J. 2019. PMID: 31162523 Free PMC article. No abstract available.
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, Gonzalez-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P; Group Scientific Document Group. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016;37:2129–2200. - PubMed
-
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD, Group E.. Fourth universal definition of myocardial infarction (2018). Eur Heart J 2019;40:237–269. - PubMed
-
- Madonna R, Van Laake LW, Davidson SM, Engel FB, Hausenloy DJ, Lecour S, Leor J, Perrino C, Schulz R, Ytrehus K, Landmesser U, Mummery CL, Janssens S, Willerson J, Eschenhagen T, Ferdinandy P, Sluijter JP.. Position Paper of the European Society of Cardiology Working Group Cellular Biology of the Heart: cell-based therapies for myocardial repair and regeneration in ischemic heart disease and heart failure. Eur Heart J 2016;37:1789–1798. - PMC - PubMed
-
- Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, Ho KK, Murabito JM, Vasan RS.. Long-term trends in the incidence of and survival with heart failure. N Engl J Med 2002;347:1397–1402. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
