

Methods and analyzers for hemoglobin measurement in clinical laboratories and field settings
- PMID: 31162693
- PMCID: PMC6709845
- DOI: 10.1111/nyas.14124
Methods and analyzers for hemoglobin measurement in clinical laboratories and field settings
Abstract
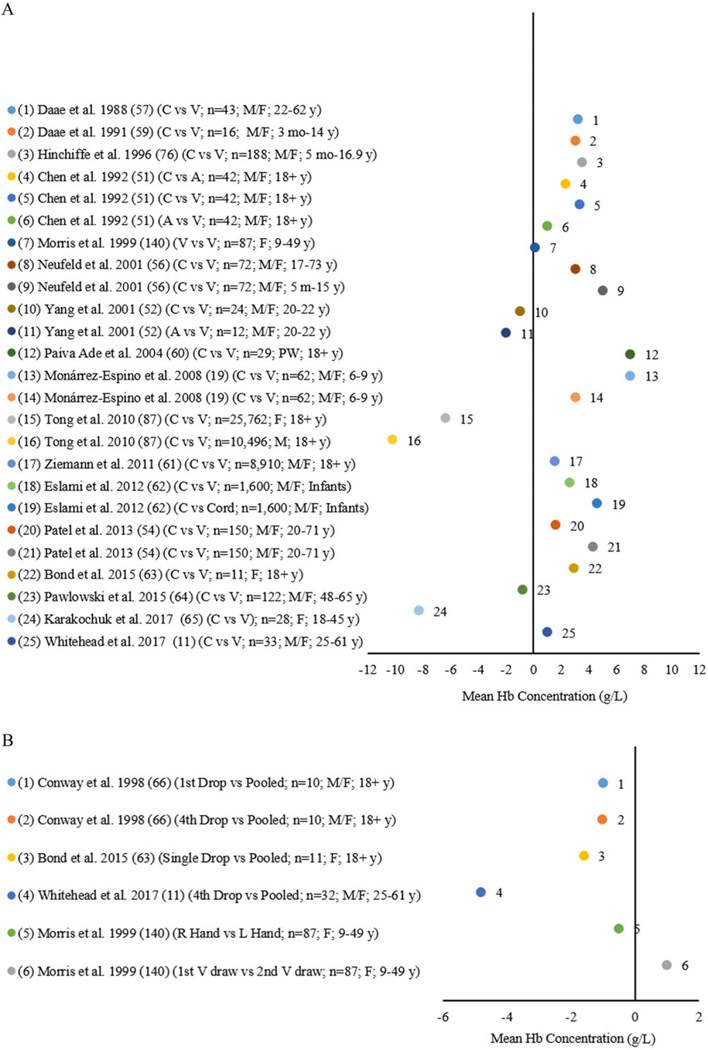
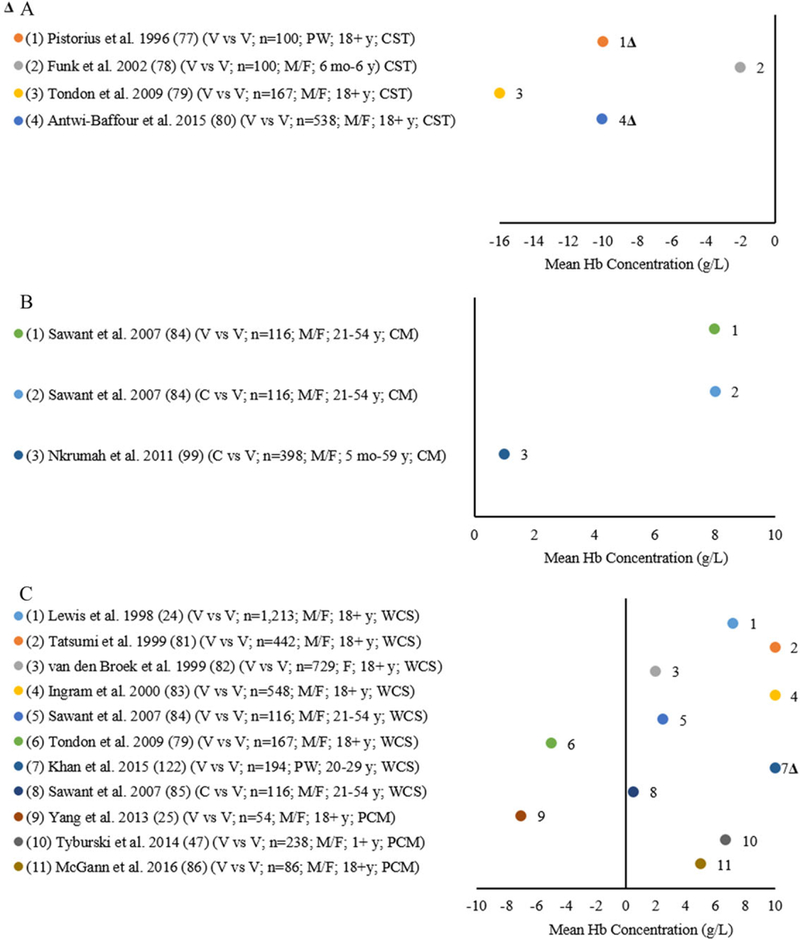
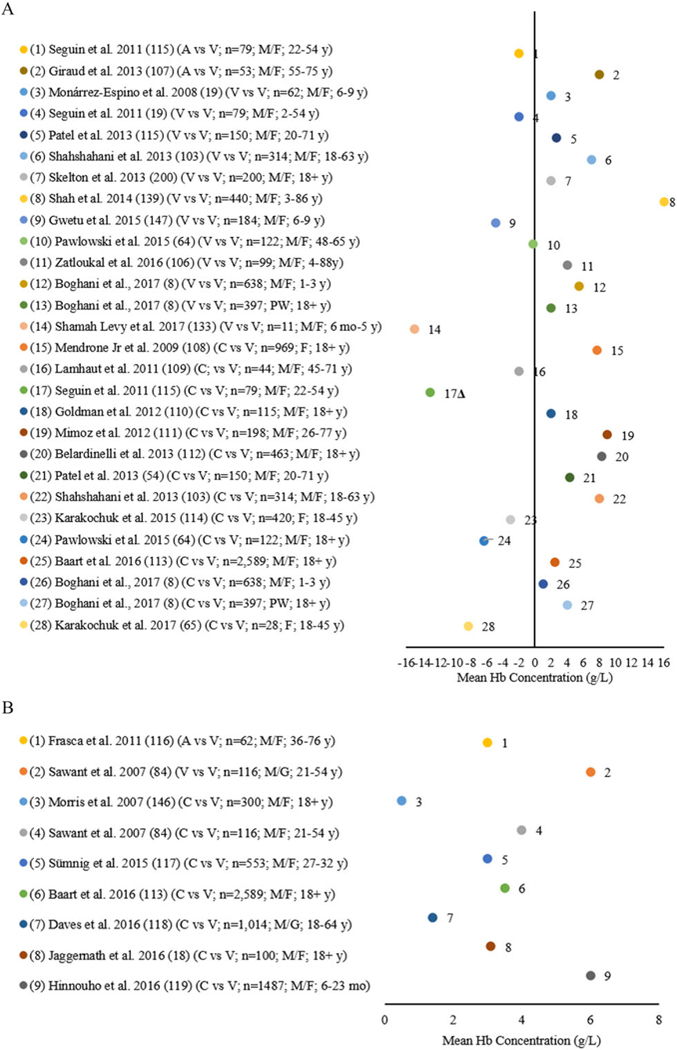
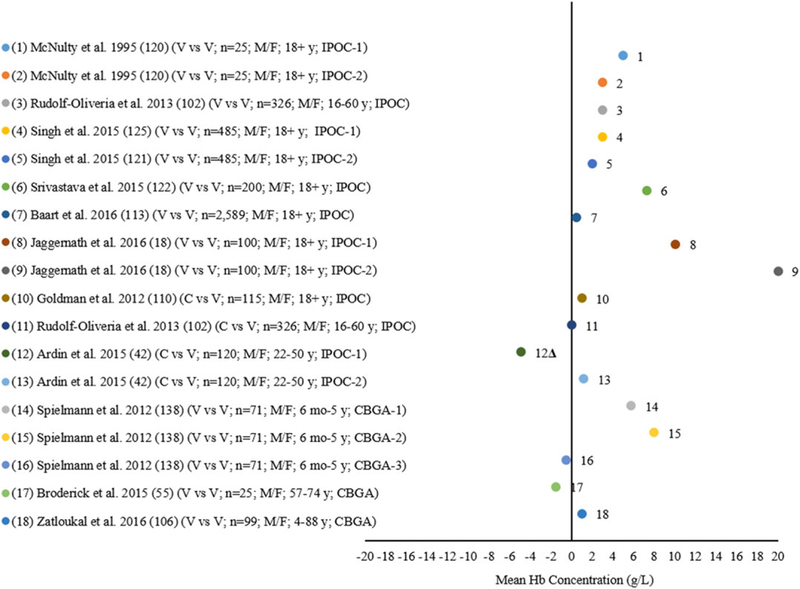
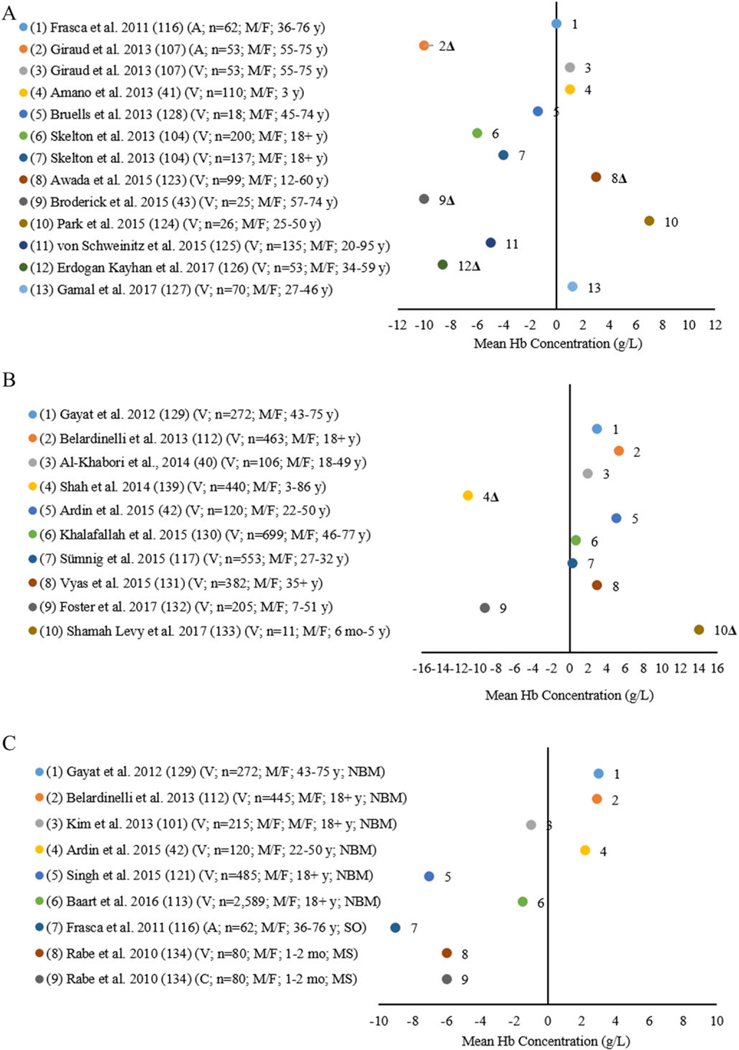
This paper describes and compares methods and analyzers used to measure hemoglobin (Hb) in clinical laboratories and field settings. We conducted a literature review for methods used to measure Hb in clinical laboratories and field settings. We described methods to measure Hb and factors influencing results. Automated hematology analyzer (AHA) was reference for all Hb comparisons using evaluation criteria of ±7% set by College of American Pathologists (CAP) and Clinical Laboratory Improvement Amendments (CLIA). Capillary fingerprick blood usually produces higher Hb concentrations compared with venous blood. Individual drops produced lower concentrations than pooled capillary blood. Compared with the AHA: (1) overall cyanmethemoglobin (1.0-8.0 g/L), WHO Colour Scale (0.5-10.0 g/L), paper-based devices (5.0-7.0 g/L), HemoCue® Hb-201 (1.0-16.0 g/L) and Hb-301 (0.5-6.0 g/L), and Masimo Pronto® (0.3-14.0 g/L) overestimated concentrations; (2) Masimo Radical®-7 both under- and overestimated concentrations (0.3-104.0 g/L); and (3) other methods underestimated concentrations (2.0-16.0 g/L). Most mean concentration comparisons varied less than ±7% of the reference. Hb measurements are influenced by several analytical factors. With few exceptions, mean concentration bias was within ±7%, suggesting acceptable performance. Appropriate, high-quality methods in all settings are necessary to ensure the accuracy of Hb measurements.This paper describes and compares methods and analyzers used to measure hemoglobin (Hb) in clinical laboratories and field settings. With few exceptions, mean concentration bias was within ±7%, suggesting acceptable performance. Appropriate, high-quality methods in all settings are necessary to ensure the accuracy of Hb measurements.
Keywords: anemia; blood collection; clinical; field; hemoglobin; variability.
Published 2019. This article is a U.S. Government work and is in the public domain in the USA.
Conflict of interest statement
Competing interests
As part of their routine work duties, the authors provide technical assistance to countries in the design, training, implementation, data management, analysis, and dissemination of public health population-based surveys, including collection of Hb and anemia.
Figures
Similar articles
-
Non-invasive hemoglobin measurement devices require refinement to match diagnostic performance with their high level of usability and acceptability.PLoS One. 2021 Jul 16;16(7):e0254629. doi: 10.1371/journal.pone.0254629. eCollection 2021. PLoS One. 2021. PMID: 34270591 Free PMC article.
-
Assessing Accuracy and Precision of Hemoglobin Determination in Venous, Capillary Pool, and Single-Drop Capillary Blood Specimens Using three Different HemoCue® Hb Models: The Multicountry Hemoglobin Measurement (HEME) Study.J Nutr. 2024 Jul;154(7):2326-2334. doi: 10.1016/j.tjnut.2024.03.019. Epub 2024 Apr 3. J Nutr. 2024. PMID: 38580209
-
Comparison of HemoCue® hemoglobin-meter and automated hematology analyzer in measurement of hemoglobin levels in pregnant women at Khartoum hospital, Sudan.Diagn Pathol. 2012 Mar 21;7:30. doi: 10.1186/1746-1596-7-30. Diagn Pathol. 2012. PMID: 22436620 Free PMC article.
-
Measurement and interpretation of hemoglobin concentration in clinical and field settings: a narrative review.Ann N Y Acad Sci. 2019 Aug;1450(1):126-146. doi: 10.1111/nyas.14003. Epub 2019 Jan 16. Ann N Y Acad Sci. 2019. PMID: 30652320 Review.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
Cited by
-
Evaluation of Hemoglobin Cutoff Levels to Define Anemia Among Healthy Individuals.JAMA Netw Open. 2021 Aug 2;4(8):e2119123. doi: 10.1001/jamanetworkopen.2021.19123. JAMA Netw Open. 2021. PMID: 34357395 Free PMC article.
-
Daily oral iron supplementation during pregnancy.Cochrane Database Syst Rev. 2024 Aug 15;8(8):CD004736. doi: 10.1002/14651858.CD004736.pub6. Cochrane Database Syst Rev. 2024. PMID: 39145520 Free PMC article.
-
A Smartphone-Based Disposable Hemoglobin Sensor Based on Colorimetric Analysis.Sensors (Basel). 2022 Dec 30;23(1):394. doi: 10.3390/s23010394. Sensors (Basel). 2022. PMID: 36616992 Free PMC article.
-
Clinical progression and outcomes of patients hospitalized with COVID-19 in humanitarian settings: A prospective cohort study in South Sudan and Eastern Democratic Republic of the Congo.PLOS Glob Public Health. 2022 Oct 19;2(10):e0000924. doi: 10.1371/journal.pgph.0000924. eCollection 2022. PLOS Glob Public Health. 2022. PMID: 36962562 Free PMC article.
-
In search of the lost blood.Blood Transfus. 2020 Jan;18(1):3-5. doi: 10.2450/2019.0007-20. Blood Transfus. 2020. PMID: 32129168 Free PMC article. No abstract available.
References
-
- World Health Organization (WHO). 2008. Worldwide prevalence of anemia, 1993–2005 In WHO Global Database on Anemia. de Benoist B, McLean E, Egli I & Cogswell M, Eds. Geneva: World Health Organization; Accessed October 25, 2018 http://whqlibdoc.who.int/publications/2008/9789241596657_eng.pdf?ua=1.
-
- McLean E, Cogswell M, Egli I, et al. 2009. Worldwide prevalence of anaemia, WHO Vitamin and Mineral Nutrition System, 1993–2005. Public Health Nutr. 12: 444–454. - PubMed
-
- World Health Organization (WHO). Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. World Health Organization; 2011. Accessed October 25, 2018 http://www.who.int/vmnis/indicators/haemoglobin.pdf?ua=1.
-
- Kassebaum NJ 2016. GBD 2013 Anemia Collaborators. The global burden of anemia. Hematol. Oncol. Clin. North Am. 30: 247–308. - PubMed
-
- Balarajan Y, Ramakrishnan U, Ozaltin E, et al. 2011. Anaemia in low-income and middle-income countries. Lancet 378: 2123–2135. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
