

Extremes of Liver Transplantation for Hepatocellular Carcinoma
- PMID: 31163668
- PMCID: PMC6616997
- DOI: 10.3390/jcm8060787
Extremes of Liver Transplantation for Hepatocellular Carcinoma
Abstract
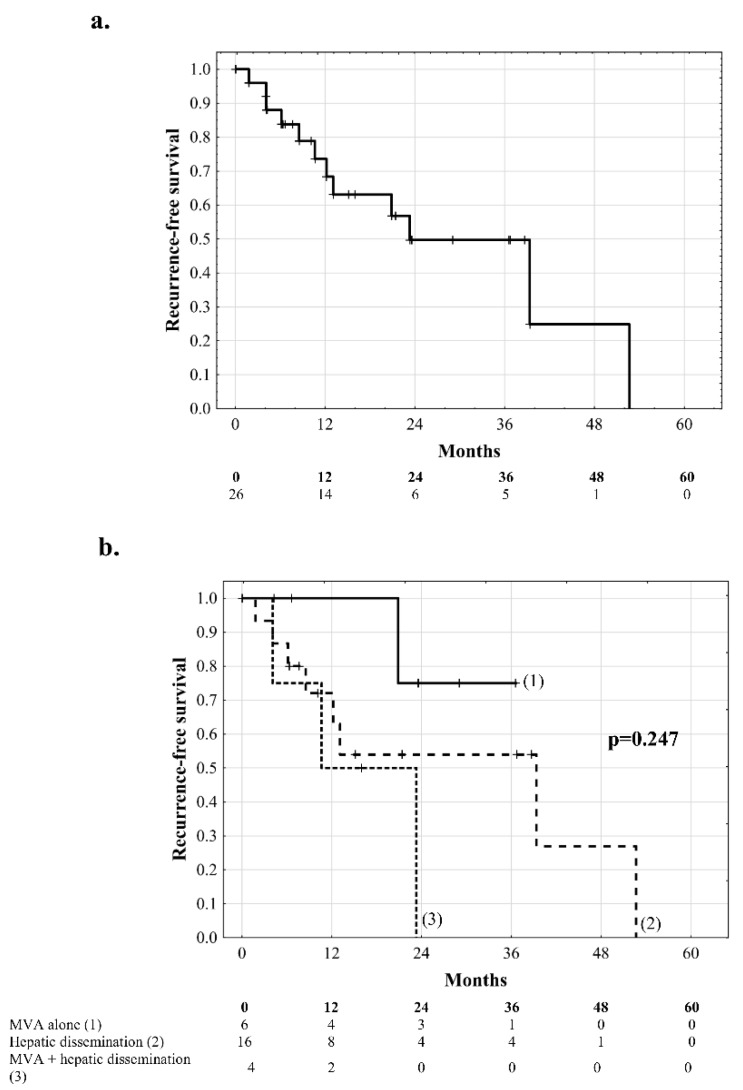
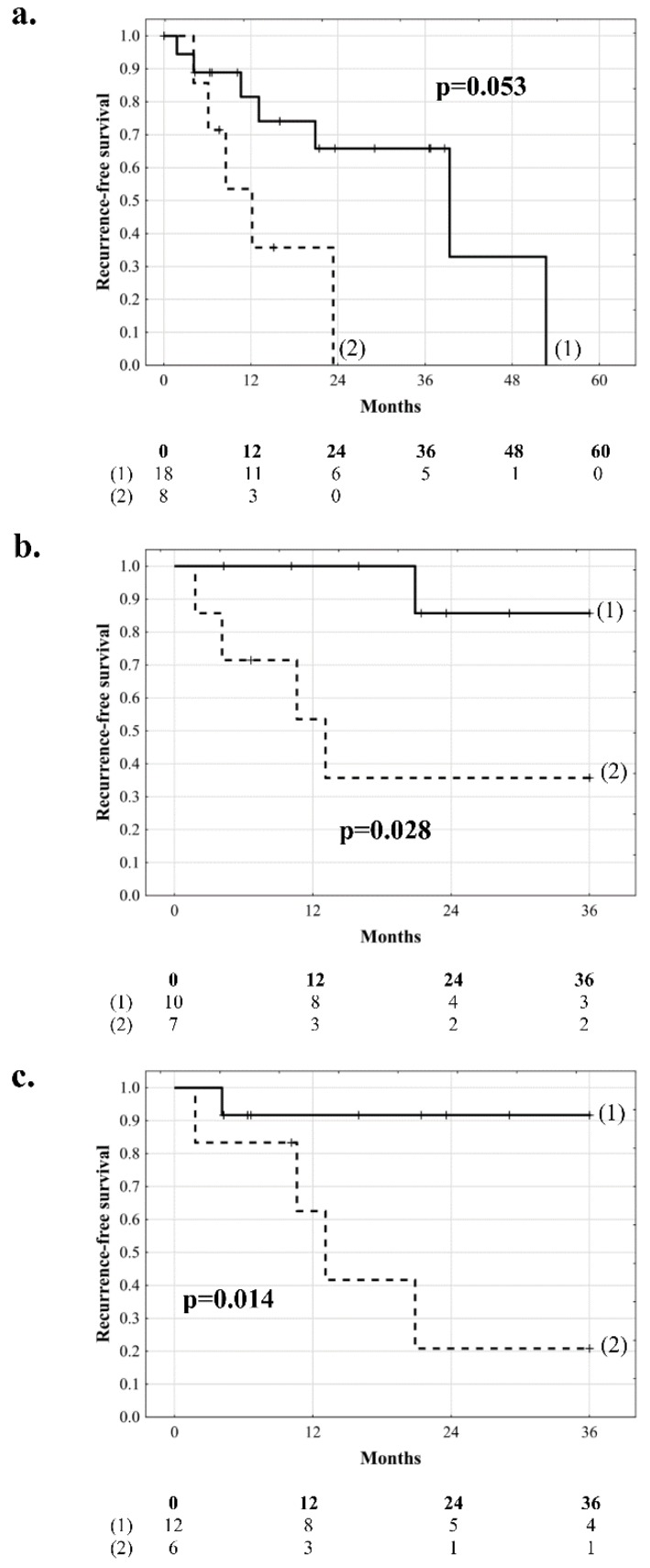
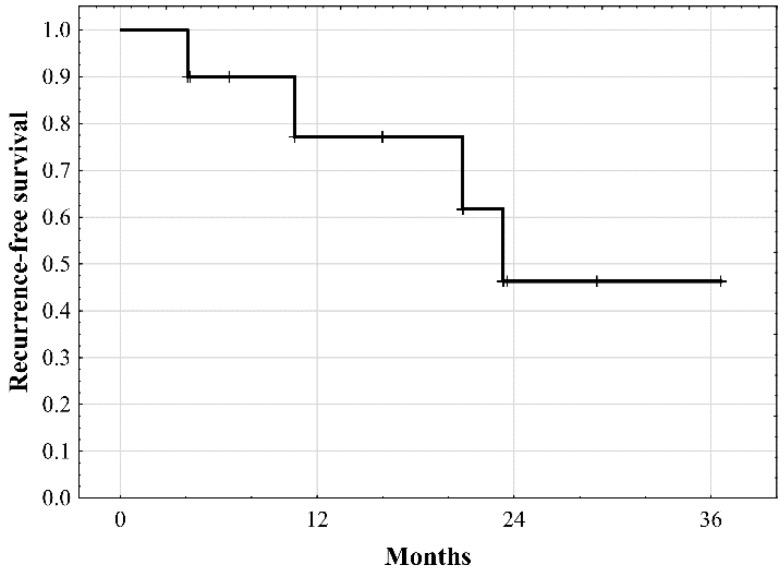
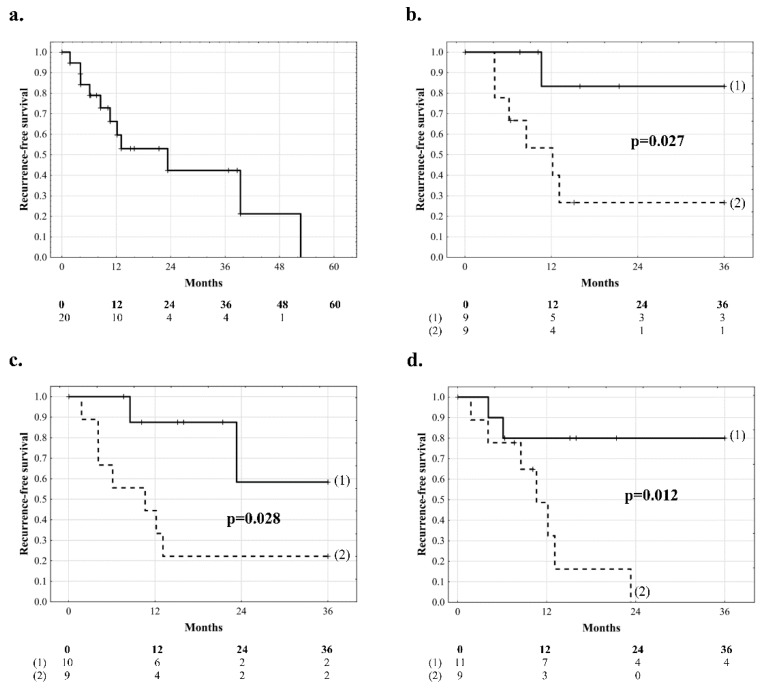
The aim of this retrospective observational study was to evaluate outcomes of patients with extremely advanced hepatocellular carcinoma (HCC) after liver transplantation. A total of 285 HCC patients after liver transplantation were screened for eligibility based on either intrahepatic dissemination (≥10 tumors) or macrovascular invasion. Tumor recurrence was the primary end-point. The study cohort comprised 26 patients. Median recurrence-free survival was 23.2 months with hepatitis B virus (HBV) infection (p = 0.038), higher AFP model score (p = 0.001), prolonged graft ischemia (p = 0.004), and younger donor age (p = 0.016) being significant risk factors. Median recurrence-free survival of HBV-negative and HBV-positive patients was 29.8 and 9.3 months, respectively (p = 0.053). In patients with macrovascular invasion, recurrence-free survival at 3 years was 46.3% with no specific predictors. Tumor size (p = 0.044), higher AFP model score (p = 0.019), prolonged graft ischemia (p = 0.016), and younger donor age (p = 0.041) were significant risk factors in patients with intrahepatic dissemination. Superior 3-year outcomes were observed in patients with intrahepatic dissemination and tumor size <3.5 cm (83.3%, p = 0.027) and HBV-negative patients with ischemia <9.7 h (85.7%, p = 0.028). In conclusion, patients with extremely advanced HCCs are remarkably heterogeneous with respect to their profile of tumor recurrence risk. This heterogeneity is largely driven by factors other than standard predictors of post-transplant HCC recurrence.
Keywords: alpha-fetoprotein; hepatocellular carcinoma; liver transplantation; tumor recurrence.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Metroticket 2.0 Model for Analysis of Competing Risks of Death After Liver Transplantation for Hepatocellular Carcinoma.Gastroenterology. 2018 Jan;154(1):128-139. doi: 10.1053/j.gastro.2017.09.025. Epub 2017 Oct 5. Gastroenterology. 2018. PMID: 28989060
-
Validation of the AFP model as a predictor of HCC recurrence in patients with viral hepatitis-related cirrhosis who had received a liver transplant for HCC.J Hepatol. 2017 Mar;66(3):552-559. doi: 10.1016/j.jhep.2016.10.038. Epub 2016 Nov 27. J Hepatol. 2017. PMID: 27899297
-
Differences in surgical outcomes between hepatitis B- and hepatitis C-related hepatocellular carcinoma: a retrospective analysis of a single North American center.Ann Surg. 2014 Oct;260(4):650-6; discussion 656-8. doi: 10.1097/SLA.0000000000000917. Ann Surg. 2014. PMID: 25203882
-
Liver transplant for hepatocellular carcinoma: experience in a Saudi population.Exp Clin Transplant. 2008 Mar;6(1):14-24. Exp Clin Transplant. 2008. PMID: 18405240
-
Evaluation of Patients With Hepatocellular Carcinomas That Do Not Produce α-Fetoprotein.JAMA Surg. 2017 Jan 1;152(1):55-64. doi: 10.1001/jamasurg.2016.3310. JAMA Surg. 2017. PMID: 27706479
Cited by
-
Managing Complex Hepatocellular Carcinoma Subtypes: Diffuse Infiltrative, Large Tumours, and Tumour Rupture-The Challenges and Strategies.J Clin Exp Hepatol. 2025 May-Jun;15(3):102505. doi: 10.1016/j.jceh.2025.102505. Epub 2025 Jan 22. J Clin Exp Hepatol. 2025. PMID: 40028241 Review.
-
Impact of Body Composition on the Risk of Hepatocellular Carcinoma Recurrence After Liver Transplantation.J Clin Med. 2019 Oct 13;8(10):1672. doi: 10.3390/jcm8101672. J Clin Med. 2019. PMID: 31614892 Free PMC article.
References
-
- Beal E.W., Tumin D., Kabir A., Moris D., Zhang X.F., Chakedis J., Washburn K., Black S., Schmidt C.M., Pawlik T.M. Cohort contributions to race- and gender-specific trends in the incidence of hepatocellular carcinoma in the USA. World J. Surg. 2018;42:835–840. doi: 10.1007/s00268-017-4194-1. - DOI - PubMed
-
- Borzio M., Dionigi E., Rossini A., Toldi A., Francica G., Fornari F., Salmi A., Farinati F., Vicari S., Marignani M., et al. Trend of improving prognosis of hepatocellular carcinoma in clinical practice: An Italian in-field experience. Dig. Dis. Sci. 2015;60:1465–1473. doi: 10.1007/s10620-014-3427-5. - DOI - PubMed
-
- Serper M., Taddei T.H., Mehta R., D’Addeo K., Dai F., Aytaman A., Baytarian M., Fox R., Hunt K., Goldberg D.S., et al. Association of provider specialty and multidisciplinary care with hepatocellular carcinoma treatment and mortality. Gastroenterology. 2017;152:1954–1964. doi: 10.1053/j.gastro.2017.02.040. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
