

Gastric Adenocarcinoma Associated with Acute Endocarditis of the Aortic Valve and Coronary Artery Disease in a 61-Year-Old Male with Multiple Comorbidities-Combined Surgical Management-Case Report
- PMID: 31163703
- PMCID: PMC6631313
- DOI: 10.3390/medicina55060242
Gastric Adenocarcinoma Associated with Acute Endocarditis of the Aortic Valve and Coronary Artery Disease in a 61-Year-Old Male with Multiple Comorbidities-Combined Surgical Management-Case Report
Abstract
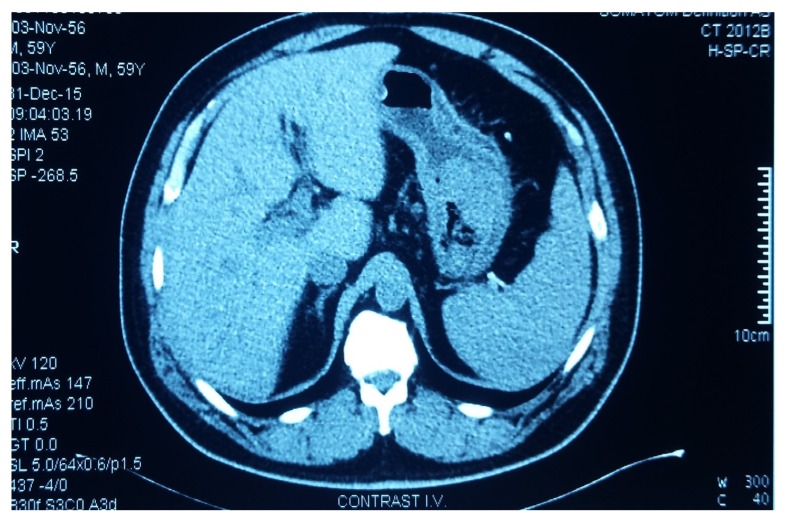
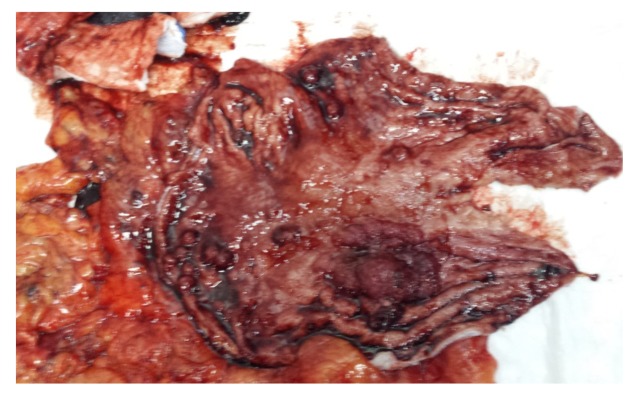
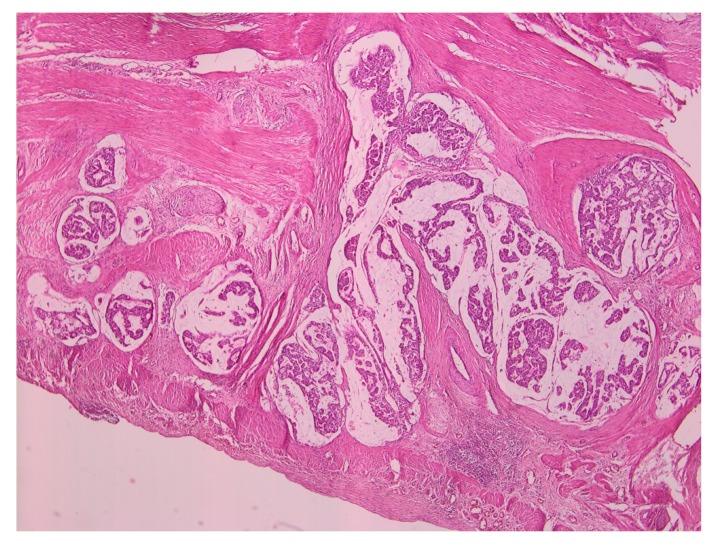
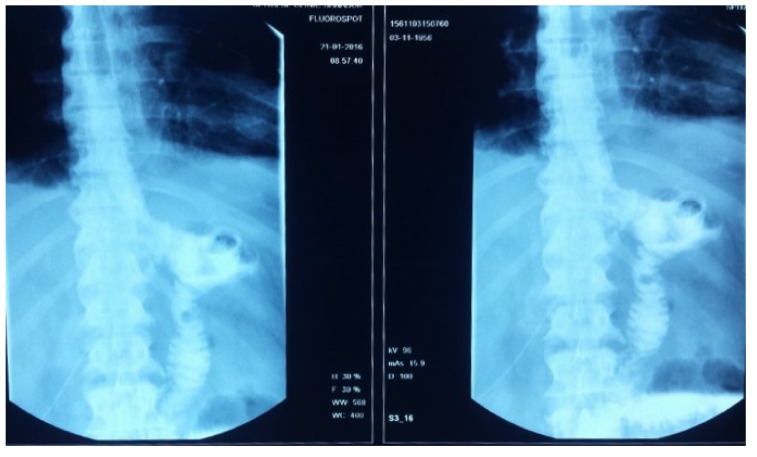
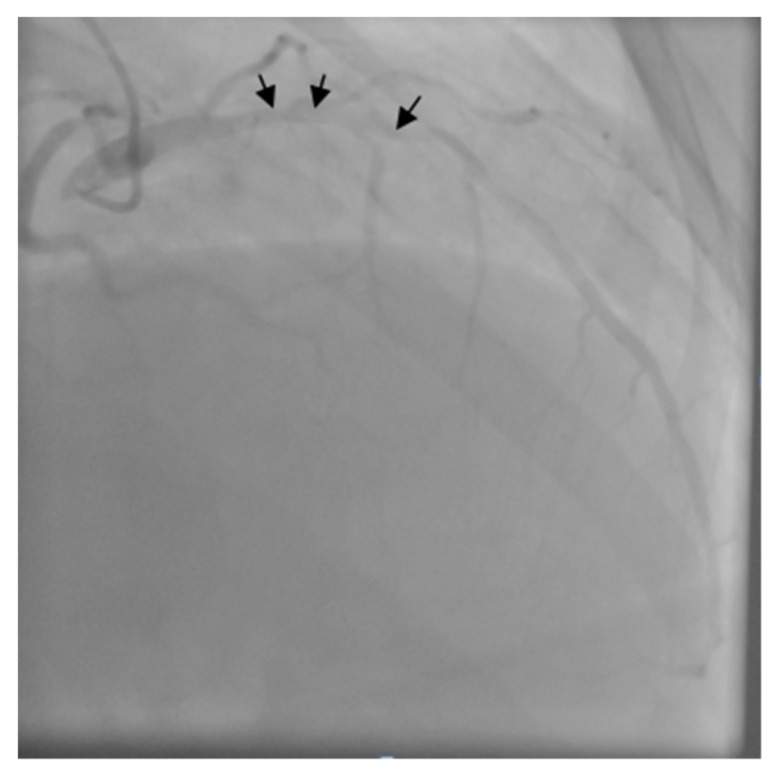
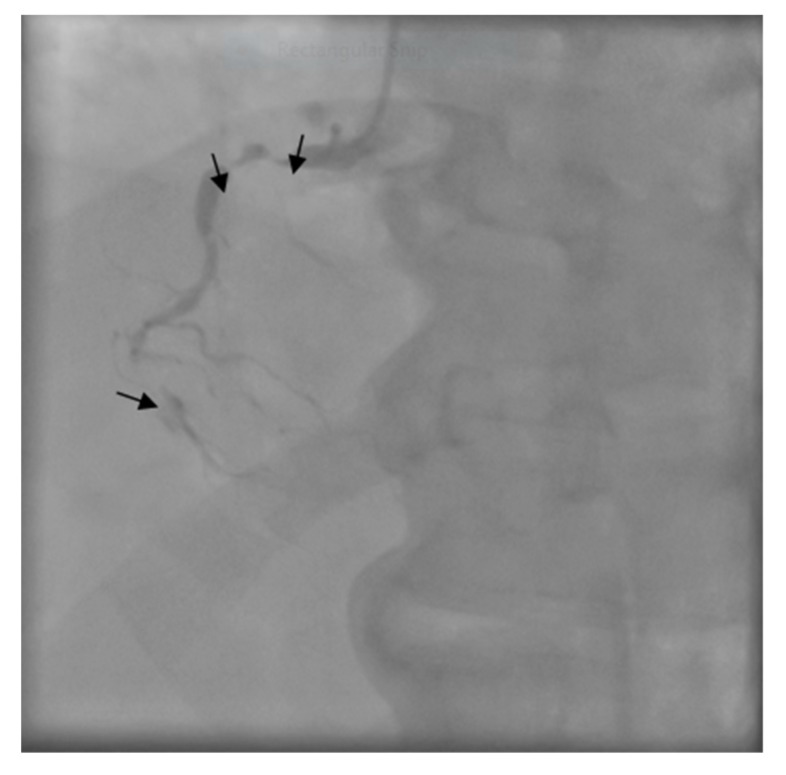
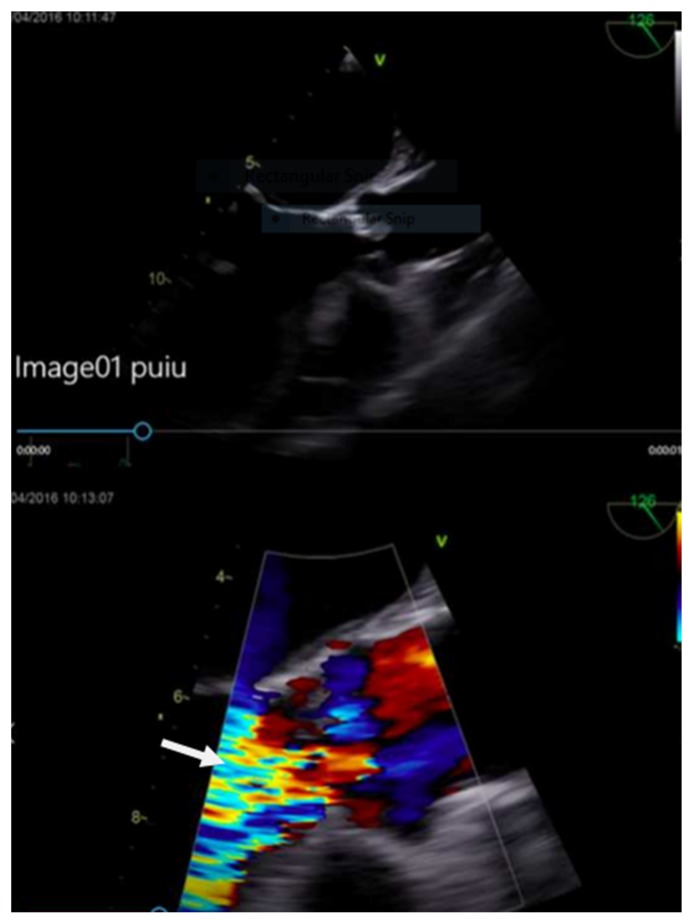
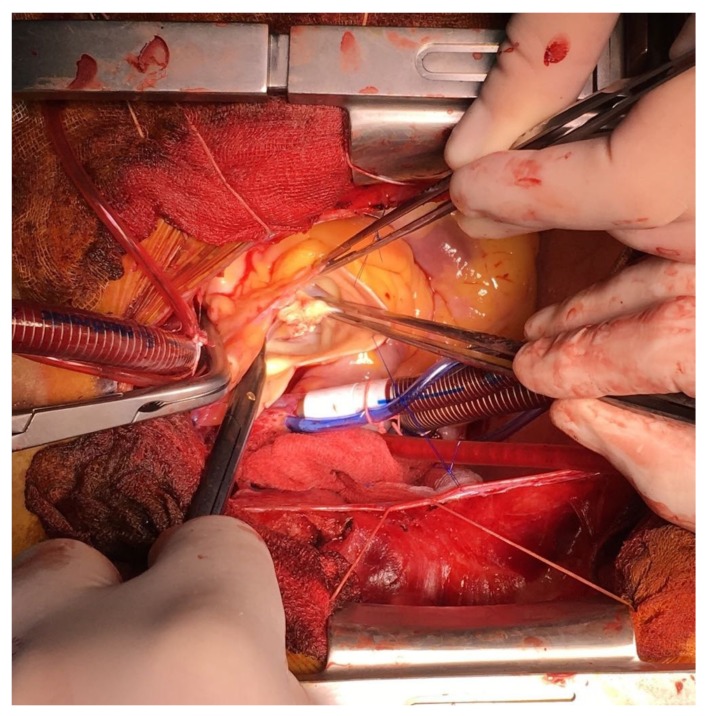
The case of a 61-year-old male with a recent total gastrectomy for a hemorrhagic gastric tumor is presented, with the important co-morbidities of type II diabetes mellitus requiring insulin, chronic hepatitis C with liver dysfunction, stage II essential hypertension, chronic stage III renal disease peripheral type II aorto-iliac disease with stage II ischemia of both legs, and chronic anemia. About one month following the gastrectomy, the patient presented with fever and acute inflammatory syndrome. Severe aortic insufficiency, aortic valvular vegetations, and positive blood cultures with Staphylococcus saprophytic were found. The diagnosis of infectious endocarditis on the aortic valve was established (positive blood cultures with echocardiographic features of vegetations, fever), and antibiotic treatment with Levofloxacin and Vancomycin was initiated. The evolution was favorable with the remission of the inflammatory syndrome and quick cessation of fever. However, the hemodynamic aspect showed progressive heart failure with acute pulmonary edema. The transesophageal echocardiographic examination confirmed the existence of severe aortic insufficiency and valvular vegetations with a left ventricular ejection fraction of 38%. The coronary angiography revealed double vessel disease. The calculated Euroscore II was 33.4%. Aortic valve replacement with porcine xenograft and double coronary artery bypass graft surgery was performed. The patient had a favorable postoperative course remaining afebrile and out of heart failure, with the markers of inflammation largely within normal limits. The left ventricular ejection fraction increased to 50%. The successful outcome of this case, represented by a rare association of cancer, endocarditis, and coronary disease, reveals the importance of the multidisciplinary teams involved in this case: gastroenterology, general surgery, cardiology, infectious diseases, cardiac surgery, and intensive care. Therefore, in such cases with high risk, complex patients, a strong collaboration between all specialties is needed to overcome all of the limitations of the patient's co-morbidities.
Keywords: acute pulmonary edema; aortic valve endocarditis; double coronary lesions; gastrectomy; gastric tumor.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Macarie C., Iliuta L., Savulescu C., Moldovan H., Gherghiceanu D.P., Vasile R., Filipescu D., Candea V. Echocardiographic predictors of embolic events in infective endocarditis. Kardiol. Pol. 2004;60:535–540. - PubMed
-
- McKenzie H., Kathyrn G., Michele S. 4-Valve Heart Disease and Right Heart Failure. J. Cardiothorac. Vasc. Anesth. 2018;32:838–845. - PubMed
-
- Fernández-Hidalgo N., Almirante B., Tornos P., González-Alujas M.T., Planes A.M., Galinanes M., Pahissa A. Immediate and long-term outcome of left-sided infective endocarditis. A 12-year prospective study from a contemporary cohort in a referral hospital. Clin. Microbiol. Infect. 2011;17:769–775. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
