

Pure stress urinary incontinence: analysis of prevalence, estimation of costs, and financial impact
- PMID: 31164133
- PMCID: PMC6549321
- DOI: 10.1186/s12894-019-0468-2
Pure stress urinary incontinence: analysis of prevalence, estimation of costs, and financial impact
Abstract
Background: The prevalence of pure stress urinary incontinence (P-SUI) and the role of urodynamic investigation (UDI) prior to surgery for stress urinary incontinence (SUI) is debated. Since the exact prevalence of P-SUI is not clear, its clinical and economic impact is not well defined. The aims of this study were to evaluate the prevalence of P-SUI in a population of women who underwent UDI for urinary incontinence (UI), also assessing: 1) the correspondence between clinical diagnosis of P-SUI and urodynamic findings; 2) the analysis of costs in terms of UDI and eventually post-UDI avoided surgical procedures.
Methods: A single cohort of women who underwent UDI for UI between January 2012 and July 2016 was prospectively collected and retrospectively analyzed. Clinical P-SUI was defined by the strict criteria of the International Continence Society. For each patient, history, physical examination and UDI were collected. The correspondence between clinical and urodynamic findings of P-SUI was analyzed. The rate of clinical P-SUI changed after performing UDI and the number of unnecessary intervention after UDI were reported. A wide cost analysis of UDIs, and the amount of surgical procedures that were believed unnecessary after UDI was reported.
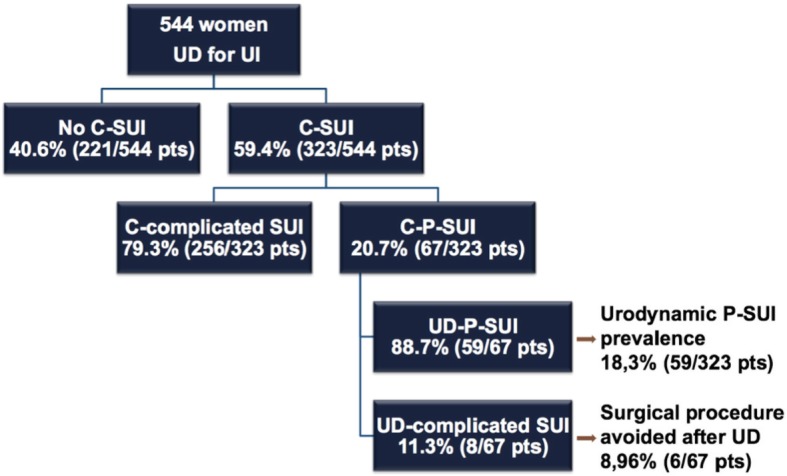
Results: Stress urinary incontinence was present in 323/544 (59.4%) patients. The prevalence of clinical P-SUI was 20.7% (67/323), while the prevalence of complicated SUI (C-SUI) was 79.3% (256/323). After UDI, diagnosis of P-SUI decreased to 18.3% (59/232). In 10.2% of cases (6/59) the scheduled middle urethral sling (MUS) was suppressed after the UDI results because 3/6 cases had detrusor overactivity and urge incontinence, in 2/6 cases SUI was treated with a conservative management, in 1/6 case an important voiding dysfunction was detected. Considering the national reimbursement in our country, the cost of each UDI was 296.5 euros and the total amount was 17,493.5 euros. So far the surgery-related savings covered 61.7-105.0% of the costs of total number of UDIs performed in the uncomplicated patients.
Conclusions: The prevalence of clinical P-SUI is relevant, involving about 20% of women with clinical SUI. Although the correspondence between clinical and urodynamic diagnosis was high, we demonstrated that UDI may help in some cases to avoid an inappropriate surgical treatment. Therefore, UDI prior to SUI surgery should be considered to achieve a correct diagnosis and a proper therapeutic strategy.
Conflict of interest statement
EFA is a member of the Editorial Board (Associate Editor) of this journal.
EFA was/is speaker honorarium/consultant for Laborie, Wellspect, Glaxo Smith Kline, Allergan, Coloplast, Astellas.
Figures
References
-
- Nager CW, Brubaker L, Litman HJ, Zyczynski HM, Varner RE, Amundsen C, Sirls LT, Norton PA, Arisco AM, Chai TC, Zimmern P, Barber MD, Dandreo KJ, Menefee SA, Kenton K, Lowder J, Richter HE, Khandwala S, Nygaard I, Kraus SR, Johnson HW, Lemack GE, Mihova M, Albo ME, Mueller E, Sutkin G, Wilson TS, Hsu Y, Rozanski TA, Rickey LM, Rahn D, Tennstedt S, Kusek JW, Gormley EA, Urinary Incontinence Treatment Network A randomized trial of urodynamic testing before stress-incontinence surgery. N Engl J Med. 2012;366(21):1987–1997. doi: 10.1056/NEJMoa1113595. - DOI - PMC - PubMed
-
- Serati M, Topazio L, Bogani G, Costantini E, Pietropaolo A, Palleschi G, Carbone A, Soligo M, Del Popolo G, Li Marzi V, Salvatore S, Finazzi Agrò E. Urodynamics useless before surgery for female stress urinary incontinence: are you sure? Results from a multicenter single nation database. Neurourol Urodyn. 2016;35(7):809–812. doi: 10.1002/nau.22804. - DOI - PubMed
-
- Van Leijsen SA, Kluivers KB, Mol BW, Broekhuis SR, Milani AL, Bongers MY, Aalders CI, Dietz V, Malmberg GG, Vierhout ME, Heesakkers JP. Can preoperative urodynamic investigation be omitted in women with stress urinary incontinence? A non-inferiority randomized controlled trial. Neurourol Urodyn. 2012;31(7):1118–1123. doi: 10.1002/nau.22230. - DOI - PubMed
-
- Norton PA, Nager CW, Brubaker L, Lemack GE, Sirls LT, Holley R, Chai TC, Kraus SR, Zyczynski H, Smith B, Stoddard A. Urinary incontinence treatment Network. The cost of preoperative urodynamics: a secondary analysis of the ValUE trial. Neurourol Urodyn. 2016;35(1):81–84. doi: 10.1002/nau.22684. - DOI - PMC - PubMed
-
- Finazzi Agrò E, Perugia C, Topazio L, Iacovelli V, Vespasiani G, Serati M. Urodynamic examinations performed before stress incontinence surgery in female patients: costs analysis in Italy. Neurourol Urodyn. 2016;35(issue S3):S51–S52.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
