

Aspergillus terreus spondylodiscitis following an abdominal stab wound: a case report
- PMID: 31164170
- PMCID: PMC6549268
- DOI: 10.1186/s13256-019-2109-5
Aspergillus terreus spondylodiscitis following an abdominal stab wound: a case report
Abstract
Background: Aspergillus terreus, a saprophytic fungus, is recognized as an emerging pathogen in various infections in humans. However, bone and joint involvement is uncommon. To the best of our knowledge, only seven cases of spondylodiscitis caused by Aspergillus terreus have been reported previously in humans. We report a case of a patient with Aspergillus terreus spondylodiscitis following an abdominal stab wound.
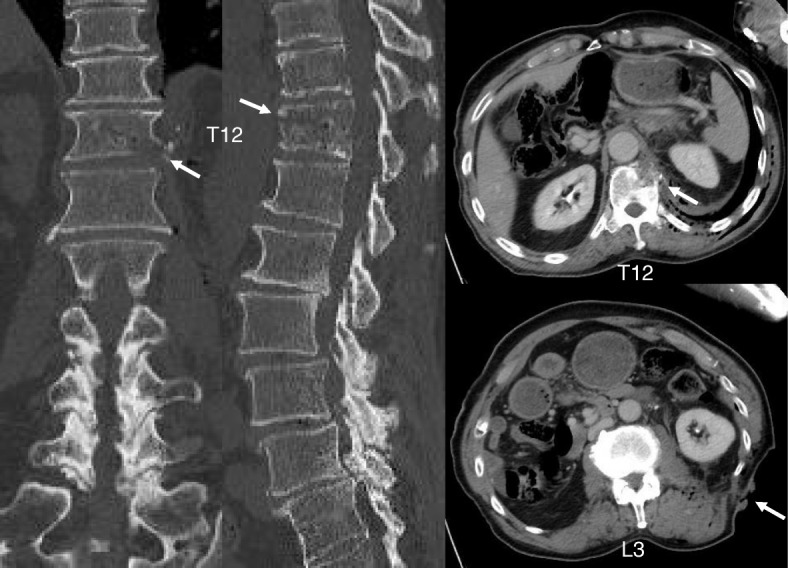
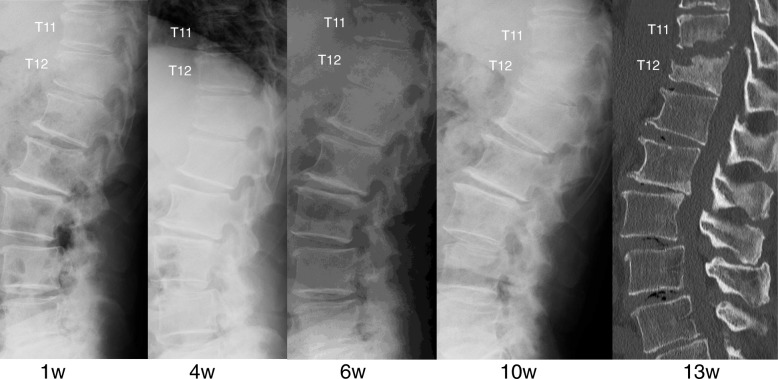
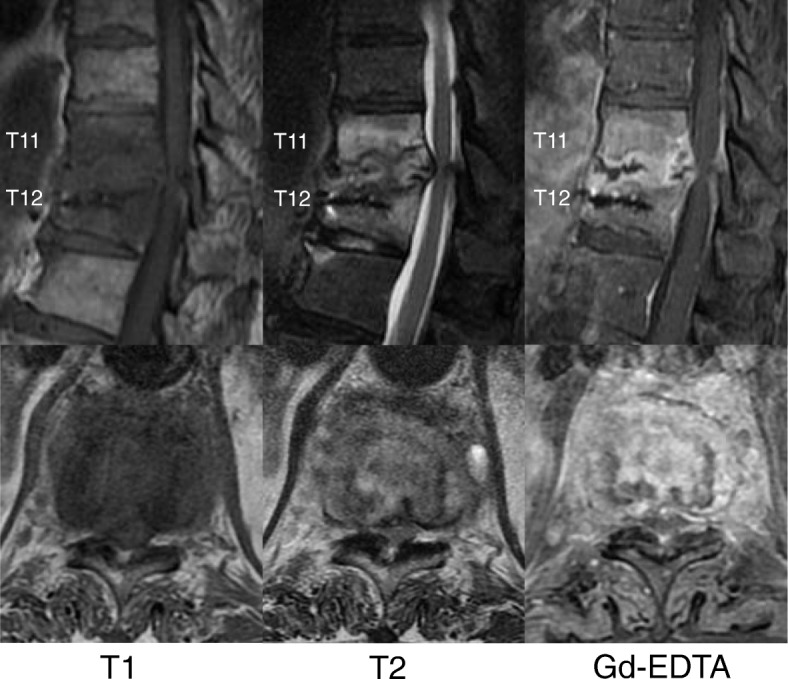
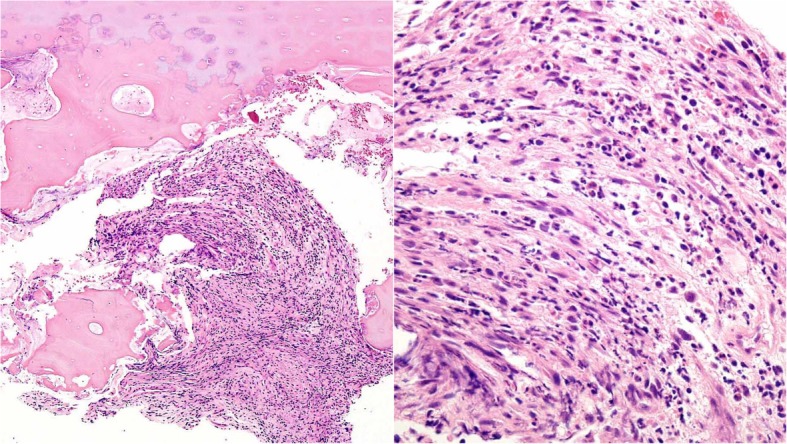
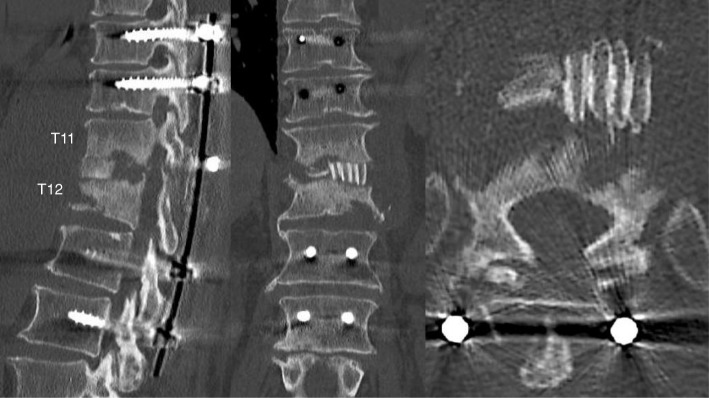
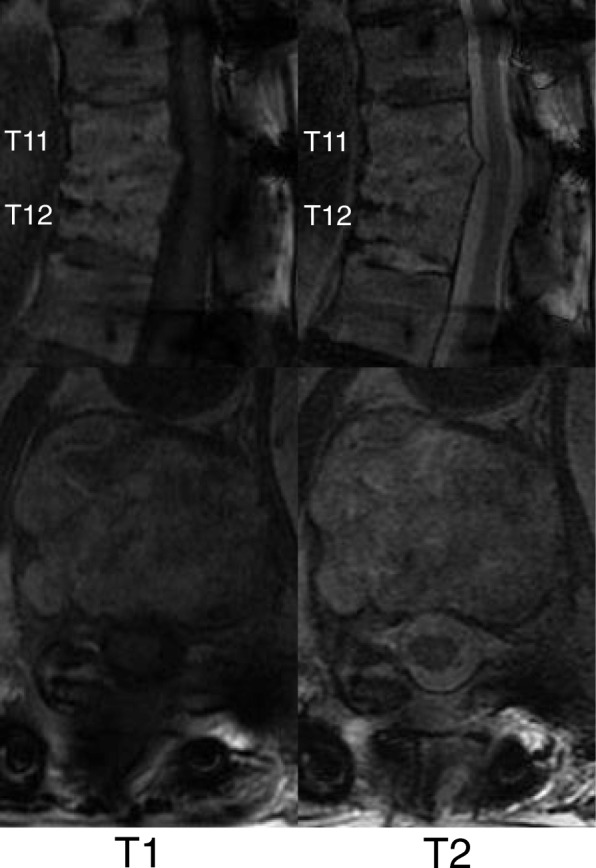
Case presentation: A 74-year-old Japanese man with no particular medical history fell from a ladder and sustained a left abdominal stab wound from an L-shaped metal peg. Computed tomography showed the trace of the L-shaped metal peg from the left abdomen to the left rib and left kidney. The scan also showed an anterolateral bone avulsion of the left side of the T12 vertebral body, as well as fractures of the L1 left transverse process and the left 10th-12th ribs. He was hospitalized and treated with conservative therapy for 6 weeks. He was readmitted to the hospital with complaints of sudden back pain, numbness of both legs, and inability to walk 13 weeks after the fall. Magnetic resonance imaging findings were typical of spondylodiscitis. Gadolinium-enhanced T1-weighted magnetic resonance imaging indicated increased signal intensity at T11-T12 vertebral bodies and severe cord compression and epidural abscess at T11-T12 associated with infiltration of soft paravertebral tissues. On the seventh day after admission, he underwent partial laminectomy at T11 and posterior fusion at T9 to L2. The result of his blood culture was negative, but Aspergillus terreus was isolated from the material of T11-T12 intervertebral disc and vertebral bodies. His Aspergillus antigen was positive in a blood examination. Histological examination showed chronic suppurative osteomyelitis. On the 35th day after admission, he underwent anterior fusion at T11 and T12 with a rib bone graft. For 5 months, voriconazole was administered, and he wore a rigid corset. Posterior partial laminectomy at T11 and anterior fusion at T11 and T12 resulted in a good clinical course. The patient's neurological dysfunction was completely recovered, and his back pain disappeared. Two years after the operation, computed tomography was performed and showed bone fusion at T11 and T12. Magnetic resonance imaging revealed no evidence of increased signal intensity at T11-T12 vertebral bodies and severe cord compression and epidural abscess at T11-T12.
Conclusions: To our knowledge, this is the first report of spondylodiscitis caused by Aspergillus terreus after an abdominal penetrating injury. The histological finding of chronic suppurative osteomyelitis and the radiological findings strongly suggested direct inoculation of Aspergillus terreus.
Keywords: Antifungals; Aspergillus terreus; Fungal infection; Open fracture of thoracic vertebra; Spondylodiscitis; Vertebral osteomyelitis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Spondylodiscitis Due to Aspergillus terreus in an Immunocompetent Host: Case Report and Literature Review.Mycopathologia. 2016 Aug;181(7-8):575-81. doi: 10.1007/s11046-016-0007-6. Epub 2016 Apr 2. Mycopathologia. 2016. PMID: 27038797
-
Cervical spondylodiscitis with epidural abscess after knife stab wounds to the neck: A case report.Injury. 2015 Aug;46(8):1684-8. doi: 10.1016/j.injury.2015.05.043. Epub 2015 May 27. Injury. 2015. PMID: 26052055
-
Salmonella Typhi Vertebral Osteomyelitis and Epidural Abscess.Case Rep Orthop. 2016;2016:6798157. doi: 10.1155/2016/6798157. Epub 2016 Mar 10. Case Rep Orthop. 2016. PMID: 27034871 Free PMC article.
-
Vertebral osteomyelitis and epidural abscess due to Aspergillus nidulans resulting in spinal cord compression: case report and literature review.J Int Med Res. 2013 Apr;41(2):502-10. doi: 10.1177/0300060513476432. Epub 2013 Feb 11. J Int Med Res. 2013. PMID: 23569017 Review.
-
Exogenous lumbar spondylodiscitis following a stabwound injury and vertebral fracture. A case report and review of the literature.Eur Spine J. 1995;4(6):357-9. doi: 10.1007/BF00300297. Eur Spine J. 1995. PMID: 8983656 Review.
Cited by
-
Aspergillus spp. osteoarticular infections: an updated systematic review on the diagnosis, treatment and outcomes of 186 confirmed cases.Med Mycol. 2022 Aug 3;60(8):myac052. doi: 10.1093/mmy/myac052. Med Mycol. 2022. PMID: 35867975 Free PMC article.
-
Aspergillus terreus Fungal Spondylodiscitis in a Healthy Patient Post-Lumbar Spine Surgery: A Rare Case Report.Asian J Neurosurg. 2025 Feb 10;20(2):383-386. doi: 10.1055/s-0045-1802624. eCollection 2025 Jun. Asian J Neurosurg. 2025. PMID: 40485804 Free PMC article.
-
Aspergillus spondylitis: case series and literature review.BMC Musculoskelet Disord. 2020 Aug 22;21(1):572. doi: 10.1186/s12891-020-03582-x. BMC Musculoskelet Disord. 2020. PMID: 32828133 Free PMC article. Review.
-
Navigating the Diagnostic Challenge of Aspergillus Spinal Epidural Abscess in an Immunocompetent Patient: A Case Report and Literature Review.Cureus. 2023 Jul 31;15(7):e42770. doi: 10.7759/cureus.42770. eCollection 2023 Jul. Cureus. 2023. PMID: 37663990 Free PMC article.
-
Isavuconazole in the Treatment of Aspergillus fumigatus Fracture-Related Infection: Case Report and Literature Review.Antibiotics (Basel). 2022 Mar 5;11(3):344. doi: 10.3390/antibiotics11030344. Antibiotics (Basel). 2022. PMID: 35326807 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
