

. 2018 Winter;54(4):10.29390/cjrt-2018-017.
doi: 10.29390/cjrt-2018-017.
Epub 2018 Feb 1.
Basic spirometry testing and interpretation for the primary care provider
Affiliations
- PMID: 31164790
- PMCID: PMC6516140
- DOI: 10.29390/cjrt-2018-017
Item in Clipboard
Basic spirometry testing and interpretation for the primary care provider
Can J Respir Ther.
2018 Winter.
Abstract
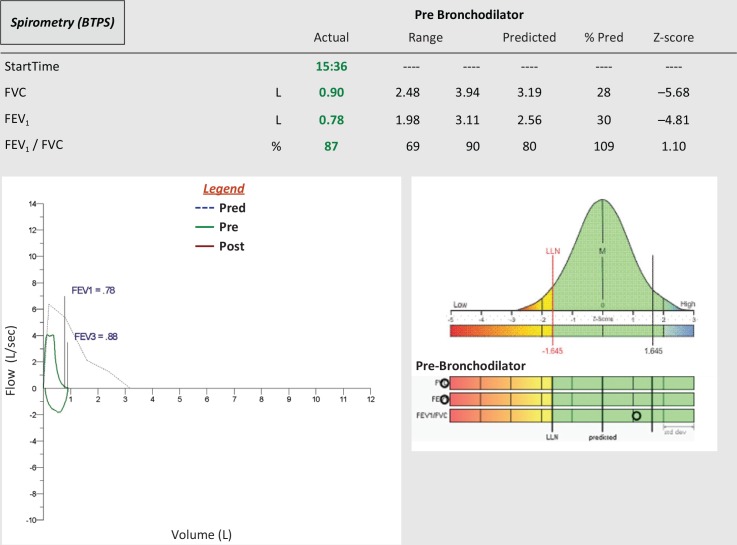
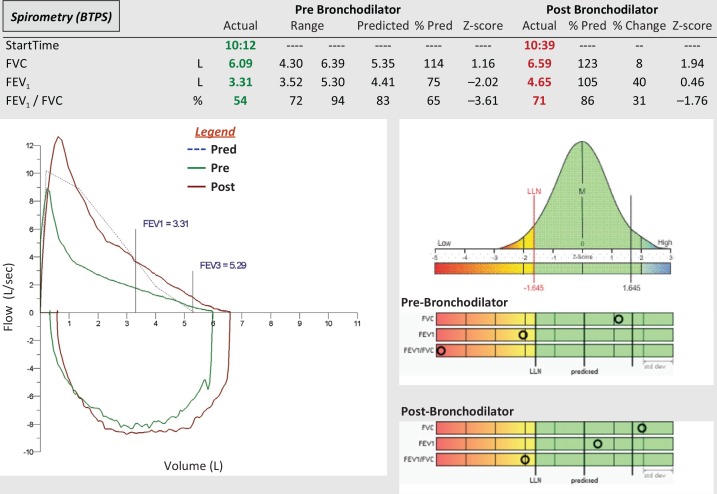
Spirometry testing plays an important role in the diagnosis and management of COPD and asthma in the primary care setting. Verifying the accuracy of the spirometer, using accurate patient demographics and appropriate reference equations, and ensuring the competency of testing personnel are key components of spirometry test interpretation. Spirometry testing plays an important role in the diagnosis and management of lung disease in the primary care setting. Spirometry interpretation should include an assessment of test quality and be based on sound statistical principals.
Keywords: lower limit of normal; primary care; respiratory function tests; spirometry.
Figures
References
-
- Global Initiative for Asthma. Global strategy for asthma management and prevention, 2018. Available at: www.ginasthma.org. [Accessed 9 July 2018].
-
- Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease, 2018 report. Available at: www.goldcopd.org. [Accessed 9 July 2018]. - PubMed
LinkOut - more resources
Full Text Sources