

Selective Recruitment of Large Lower Lobe Atelectasis on Donor Back Table in Rejected Donor Lungs
- PMID: 31165088
- PMCID: PMC6511443
- DOI: 10.1097/TXD.0000000000000889
Selective Recruitment of Large Lower Lobe Atelectasis on Donor Back Table in Rejected Donor Lungs
Abstract
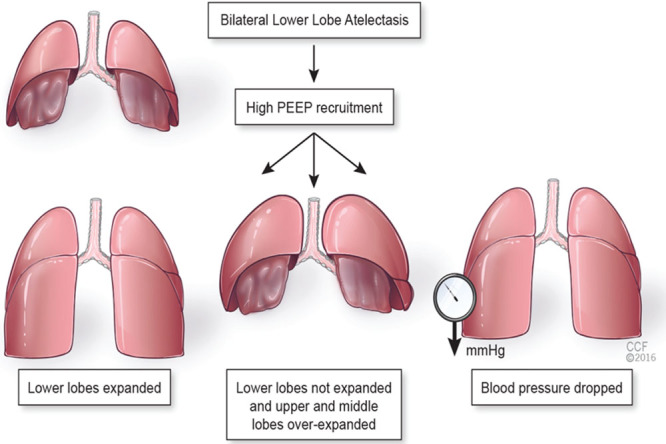
Background: Large atelectatic areas in donor lungs are frequently resistant to standard recruitment maneuvers, producing a tenaciously low PO2/FiO2 ratio. The aim of this study is to investigate the optimal protocol for the recruitment of large atelectatic areas in the context of ex vivo lung perfusion (EVLP).
Methods: Seventeen rejected lungs with large lower lobe atelectasis (≥40%) were divided into 2 groups: manual resuscitation (n = 5) and selective recruitment (n = 12). Transplant suitability was then evaluated in cellular EVLP. In the manual resuscitation group, following bronchoscopy, if the conventional recruitment maneuver was not successful, a bagging technique was utilized to resolve atelectasis in EVLP. In the selective recruitment group, a pediatric endotracheal tube was introduced to the lower lobe bronchus on the back table of the donor hospital. Selective recruitment of the lower lobe was accomplished while keeping peak inspiratory pressure <30 cm H2O for 30 seconds.
Results: The average atelectasis size and lung weight in 17 donor lungs was 75.4 ± 20.6% and 960 ± 221 g, respectively. There were no significant differences between the 2 groups in all donor variables, except cold ischemic time (P = 0.001, 5.2 ± 0.5 versus 6.4 ± 0.7 hours). The selective recruitment group was associated with better transplant suitability (P = 0.035, 75% versus 20%), better PO2/FiO2 ratio (P = 0.186, 324 ± 89 versus 258 ± 87 mm Hg), lower lung weight (P = 0.057, 997.9 ± 229.2 versus 1377.2 ± 452.9 g), and better pathological score (P < 0.05, 1.0 ± 1.3 versus 2.8 ± 0.8) than the manual resuscitation group.
Conclusion: A selective recruitment procedure is a safe and effective method of eliminating large atelectasis before EVLP.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



References
-
- Gunnarsson L, Tokics L, Gustavsson H, et al. Influence of age on atelectasis formation and gas exchange impairment during general anaesthesia. Br J Anaesth. 1991;66:423. - PubMed
-
- Brooks-Brunn JA. Postoperative atelectasis and pneumonia: risk factors. Am J Crit Care. 1995;4:340. - PubMed
-
- Eichenberger A, Proietti S, Wicky S, et al. Morbid obesity and postoperative pulmonary atelectasis: an underestimated problem. Anesth Analg. 2002;95:1788. - PubMed
-
- Duggan M, Kavanagh BP. Pulmonary atelectasis: a pathogenic perioperative entity. Anesthesiology. 2005;102:838. - PubMed
-
- Parry A, Higgins R, Wheeldon D, et al. The contribution of donor management and modified cold blood lung perfusate to post-transplant lung function. J Heart Lung Transplant. 1999;18:121. - PubMed
LinkOut - more resources
Full Text Sources
