

Systematic review with meta-analysis: association between Helicobacter pylori CagA seropositivity and odds of inflammatory bowel disease
- PMID: 31165513
- PMCID: PMC7393806
- DOI: 10.1111/apt.15306
Systematic review with meta-analysis: association between Helicobacter pylori CagA seropositivity and odds of inflammatory bowel disease
Abstract
Background: Accumulating data support a protective role of Helicobacter pylori against inflammatory bowel diseases (IBD), which might be mediated by strain-specific constituents, specifically cagA expression.
Aim: To perform a systematic review and meta-analysis to more clearly define the association between CagA seropositivity and IBD.
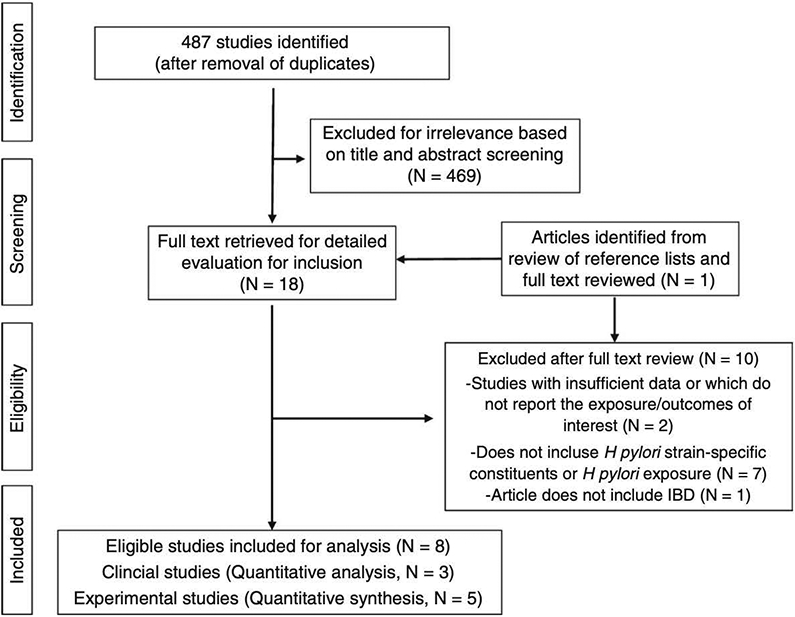
Methods: We identified comparative studies that included sufficient detail to determine the odds or risk of IBD, Crohn's disease (CD) or ulcerative colitis (UC) amongst individuals with vs without evidence of cagA expression (eg CagA seropositivity). Estimates were pooled using a random effects model.
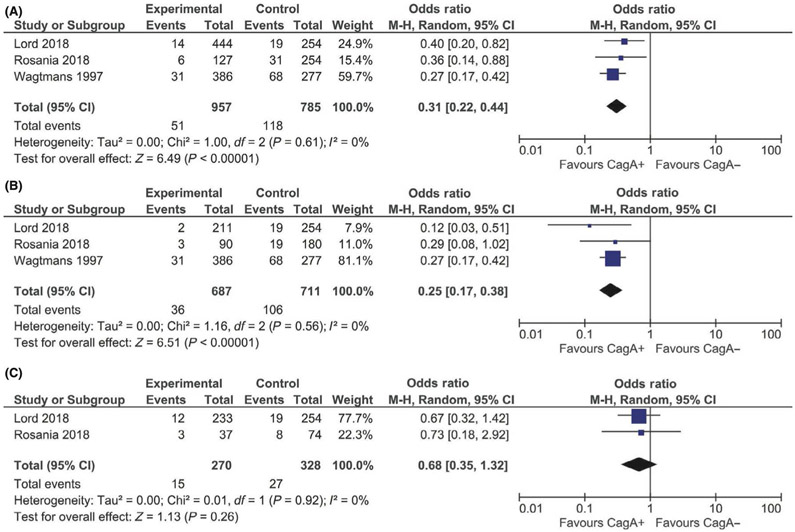
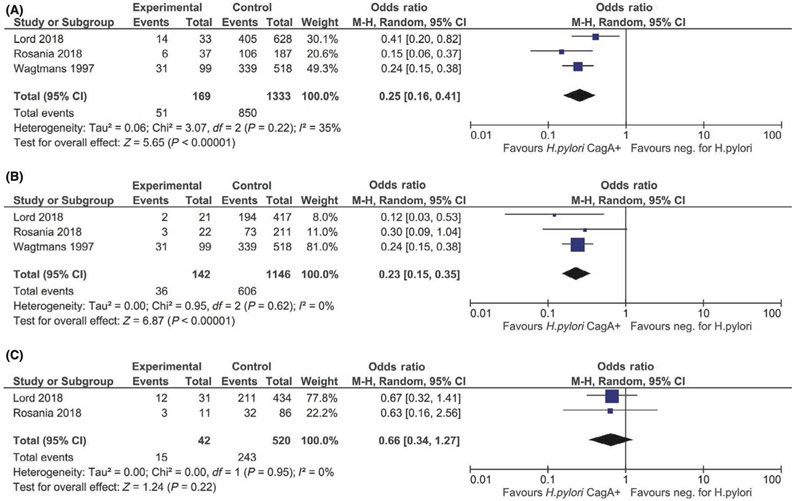
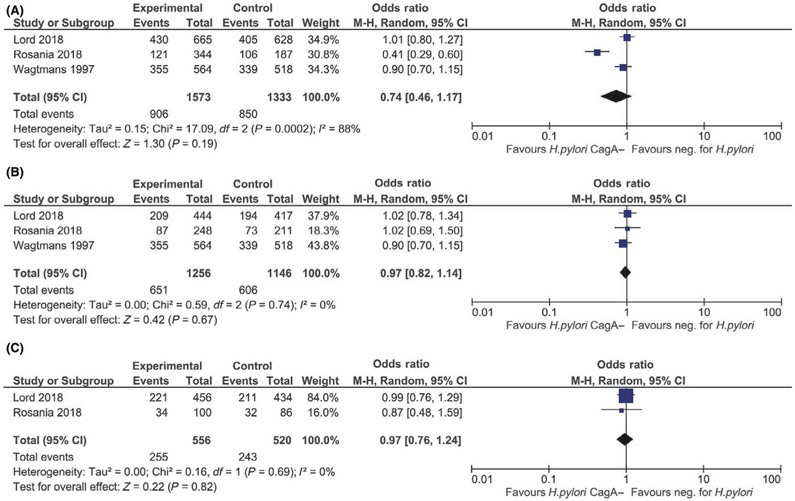
Results: Three clinical studies met inclusion criteria. cagA expression was represented by CagA seropositivity in all studies. Compared to CagA seronegativity overall, CagA seropositivity was associated with lower odds of IBD (OR 0.31, 95% CI 0.21-0.44) and CD (OR 0.25, 95% CI 0.17-0.38), and statistically nonsignificant lower odds for UC (OR 0.68, 95% CI 0.35-1.32). Similarly, compared to H pylori non-exposed individuals, H pylori exposed, CagA seropositive individuals had lower odds of IBD (OR 0.26, 95% CI 0.16-0.41) and CD (OR 0.23, 95% CI 0.15-0.35), but not UC (OR 0.66, 0.34-1.27). However, there was no significant difference in the odds of IBD, CD or UC between H pylori exposed, CagA seronegative and H pylori non-exposed individuals.
Conclusion: We found evidence for a significant association between CagA seropositive H pylori exposure and reduced odds of IBD, particularly CD, but not for CagA seronegative H pylori exposure. Additional studies are needed to confirm these findings and define underlying mechanisms.
© 2019 John Wiley & Sons Ltd.
Conflict of interest statement
Figures
Similar articles
-
Evaluation of western blot CagA seropositivity in Helicobacter pylori-seropositive and -seronegative subjects.Clin Diagn Lab Immunol. 2005 Feb;12(2):304-9. doi: 10.1128/CDLI.12.2.304-309.2005. Clin Diagn Lab Immunol. 2005. PMID: 15699426 Free PMC article.
-
The prevalence of Helicobacter pylori gastritis in newly diagnosed children with inflammatory bowel disease.Helicobacter. 2014 Oct;19(5):400-5. doi: 10.1111/hel.12141. Epub 2014 May 14. Helicobacter. 2014. PMID: 24827117
-
Seroprevalence of Helicobacter pylori infection in inflammatory bowel disease: is Helicobacter pylori infection a protective factor?Scand J Gastroenterol. 2001 Dec;36(12):1295-300. doi: 10.1080/003655201317097155. Scand J Gastroenterol. 2001. PMID: 11761020
-
The association between Helicobacter pylori infection and inflammatory bowel disease in children: A systematic review with meta-analysis.Medicine (Baltimore). 2023 Sep 8;102(36):e34882. doi: 10.1097/MD.0000000000034882. Medicine (Baltimore). 2023. PMID: 37682136 Free PMC article.
-
Association between Helicobacter pylori and pancreatic cancer risk: a meta-analysis.Cancer Causes Control. 2015 Jul;26(7):1027-35. doi: 10.1007/s10552-015-0595-3. Epub 2015 May 8. Cancer Causes Control. 2015. PMID: 25951801
Cited by
-
Bibliometric analysis of the correlation between H. pylori and inflammatory bowel disease.JGH Open. 2024 Aug 15;8(8):e70014. doi: 10.1002/jgh3.70014. eCollection 2024 Aug. JGH Open. 2024. PMID: 39148512 Free PMC article. Review.
-
Debate on the relationship between Helicobacter pylori infection and inflammatory bowel disease: a bibliometric analysis.Front Microbiol. 2024 Nov 6;15:1479941. doi: 10.3389/fmicb.2024.1479941. eCollection 2024. Front Microbiol. 2024. PMID: 39569001 Free PMC article.
-
Helicobacter pylori and unignorable extragastric diseases: Mechanism and implications.Front Microbiol. 2022 Aug 4;13:972777. doi: 10.3389/fmicb.2022.972777. eCollection 2022. Front Microbiol. 2022. PMID: 35992650 Free PMC article. Review.
-
Helicobacter Pylori and Autoimmune Diseases: Involving Multiple Systems.Front Immunol. 2022 Feb 10;13:833424. doi: 10.3389/fimmu.2022.833424. eCollection 2022. Front Immunol. 2022. PMID: 35222423 Free PMC article. Review.
-
Exosomal CagA from Helicobacter pylori aggravates intestinal epithelium barrier dysfunction in chronic colitis by facilitating Claudin-2 expression.Gut Pathog. 2022 Mar 24;14(1):13. doi: 10.1186/s13099-022-00486-0. Gut Pathog. 2022. PMID: 35331316 Free PMC article.
References
-
- Torres J, Mehandru S, Colombel J-F, Peyrin-Biroulet L. Crohn’s disease. The Lancet 2017; 389: 1741–1755. - PubMed
-
- Hooi JKY, Lai WY, Ng WK, et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology 2017; 153: 420–429. - PubMed
-
- Breurec S, Raymond J, Thiberge J-M, et al. Impact of human migrations on diversity of Helicobacter pylori in Cambodia and New Caledonia. Helicobacter 2013; 18: 249–261. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous