

Postoperative Delirium and Postoperative Cognitive Dysfunction: Overlap and Divergence
- PMID: 31166241
- PMCID: PMC6692220
- DOI: 10.1097/ALN.0000000000002729
Postoperative Delirium and Postoperative Cognitive Dysfunction: Overlap and Divergence
Abstract
Background: Postoperative delirium and postoperative cognitive dysfunction share risk factors and may co-occur, but their relationship is not well established. The primary goals of this study were to describe the prevalence of postoperative cognitive dysfunction and to investigate its association with in-hospital delirium. The authors hypothesized that delirium would be a significant risk factor for postoperative cognitive dysfunction during follow-up.
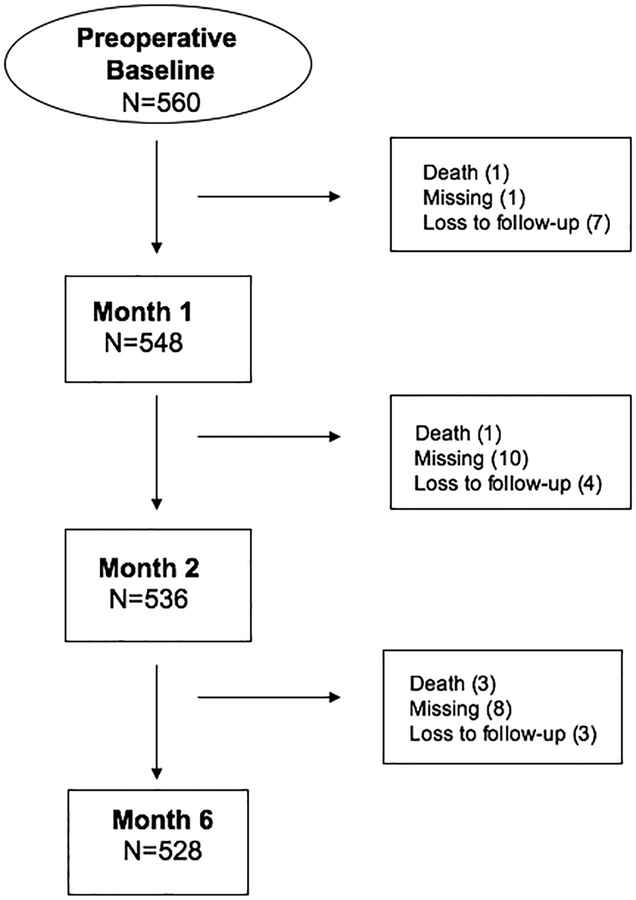
Methods: This study used data from an observational study of cognitive outcomes after major noncardiac surgery, the Successful Aging after Elective Surgery study. Postoperative delirium was evaluated each hospital day with confusion assessment method-based interviews supplemented by chart reviews. Postoperative cognitive dysfunction was determined using methods adapted from the International Study of Postoperative Cognitive Dysfunction. Associations between delirium and postoperative cognitive dysfunction were examined at 1, 2, and 6 months.
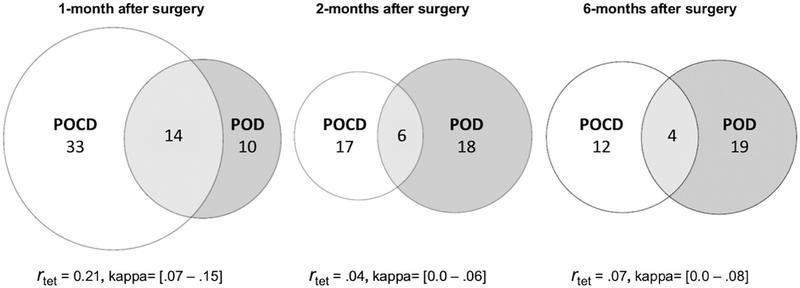
Results: One hundred thirty-four of 560 participants (24%) developed delirium during hospitalization. Slightly fewer than half (47%, 256 of 548) met the International Study of Postoperative Cognitive Dysfunction-defined threshold for postoperative cognitive dysfunction at 1 month, but this proportion decreased at 2 months (23%, 123 of 536) and 6 months (16%, 85 of 528). At each follow-up, the level of agreement between delirium and postoperative cognitive dysfunction was poor (kappa less than .08) and correlations were small (r less than .16). The relative risk of postoperative cognitive dysfunction was significantly elevated for patients with a history of postoperative delirium at 1 month (relative risk = 1.34; 95% CI, 1.07-1.67), but not 2 months (relative risk = 1.08; 95% CI, 0.72-1.64), or 6 months (relative risk = 1.21; 95% CI, 0.71-2.09).
Conclusions: Delirium significantly increased the risk of postoperative cognitive dysfunction in the first postoperative month; this relationship did not hold in longer-term follow-up. At each evaluation, postoperative cognitive dysfunction was more common among patients without delirium. Postoperative delirium and postoperative cognitive dysfunction may be distinct manifestations of perioperative neurocognitive deficits.
Conflict of interest statement
Figures
Comment in
-
The Devil Is in the Details: Comparison of Postoperative Delirium and Neurocognitive Dysfunction.Anesthesiology. 2019 Sep;131(3):456-458. doi: 10.1097/ALN.0000000000002823. Anesthesiology. 2019. PMID: 31166239 Free PMC article. No abstract available.
References
-
- U.S. Census Bureau PD. Annual Estimates of the Resident Population for Selected Age Groups by Sex for the United States, States, Counties, and Puerto Rico Commonwealth and Municipios: April 1, 2010. to July 1, 2014.
-
- McDermott KFW, Elixhauser A Overview of Operating Room Procedures During Inpatient Stays in US Hospitals, 2014: Statistical Brief# 233. In. Rockville, MD: Agency for Healthcare Research and Quality. - PubMed
-
- Moller JT, Cluitmans P, Rasmussen LS, Houx P, Rasmussen H, Canet J, Rabbitt P, Jolles J, Larsen K, Hanning CD, Langeron O, Johnson T, Lauven PM, Kristensen PA, Biedler A, van Beem H, Fraidakis O, Silverstein JH, Beneken JE, Gravenstein JS. Long-term postoperative cognitive dysfunction in the elderly ISPOCD1 study. ISPOCD investigators. International Study of Post-Operative Cognitive Dysfunction. Lancet. 1998;351(9106):857–861. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 AG044518/AG/NIA NIH HHS/United States
- K08 MH116135/MH/NIMH NIH HHS/United States
- R03 AG061582/AG/NIA NIH HHS/United States
- K24 AG035075/AG/NIA NIH HHS/United States
- K07 AG041835/AG/NIA NIH HHS/United States
- R01 AG058648/AG/NIA NIH HHS/United States
- K01 AG057836/AG/NIA NIH HHS/United States
- P01 AG031720/AG/NIA NIH HHS/United States
- T32 AG023480/AG/NIA NIH HHS/United States
- UL1 TR001102/TR/NCATS NIH HHS/United States
- R01 AG030618/AG/NIA NIH HHS/United States
- R24 AG054259/AG/NIA NIH HHS/United States
- R03 AG050878/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
