

Consensus on the treatment of autoimmune bullous dermatoses: pemphigus vulgaris and pemphigus foliaceus - Brazilian Society of Dermatology
- PMID: 31166407
- PMCID: PMC6544031
- DOI: 10.1590/abd1806-4841.2019940206
Consensus on the treatment of autoimmune bullous dermatoses: pemphigus vulgaris and pemphigus foliaceus - Brazilian Society of Dermatology
Abstract
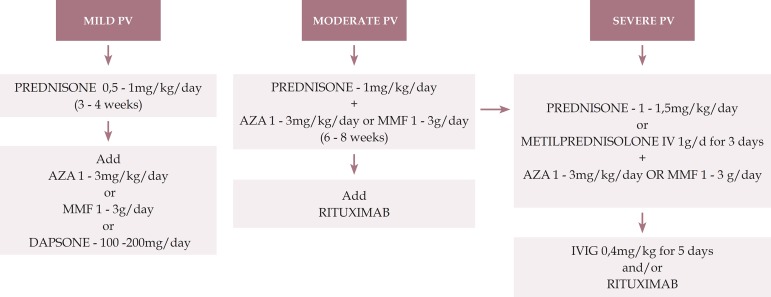
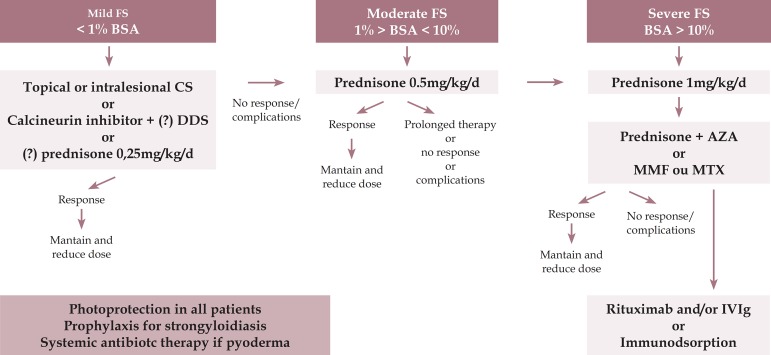
Pemphigus are intraepidermal autoimmune bullous dermatoses that occur with lesions on the skin and / or mucous membranes. The most frequent types are pemphigus vulgaris and pemphigus foliaceus (classic and endemic). This consensus aims to present a complete and updated review of the treatment of these two more frequent forms of pemphigus, based on the literature and the personal experience of the authors. In moderate and severe cases of pemphigus vulgaris and foliaceus, systemic corticosteroid therapy (prednisone or prednisolone) is the treatment of choice. Adjuvant drugs, usually immunosuppressive drugs (azathioprine, mycophenolate mofetil, methotrexate, cyclophosphamide) may be prescribed as corticosteroid sparers in refractory cases or with contraindications to corticosteroids to minimize side effects. In severe and nonresponsive cases, corticosteroids in the form of intravenous pulse therapy, immunoglobulin and plasmapheresis / immunoadsorption can be administered. Immunobiological drugs, particularly rituximab, appear as a promising alternative. For milder cases, smaller doses of oral corticosteroid, dapsone and topical corticosteroids are options. At the end flowcharts are presented as suggestions for a therapeutic approach for patients with pemphigus vulgaris and pemphigus foliaceus.
Conflict of interest statement
Conflict of interest: None.
Figures
References
-
- Kridin K, Sagi SZ, Bergman R. Mortality and cause of death in Israeli patients with pemphigus. Acta Derm Venereol. 2017;97:607–611. - PubMed
-
- Hsu DY, Brieva J, Sinha AA, Langan SM, Silverberg JI. Comorbidities and inpatient mortality for pemphigus in the USA. Br J Dermatol. 2016;174:1290–1298. - PubMed
-
- Di Zenzo G, Amber KT, Sayar BS, Müller EJ, Borradori L. Immune response in pemphigus and beyond: progresses and emerging concepts. Semin Immunopathol. 2016;38:57–74. - PubMed
-
- Pan M, Liu X, Zheng J. The pathogenic role of autoantibodies in pemphigus vulgaris. Clin Exp Dermatol. 2011;36:703–707. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
