

Surgical interventions for women with stress urinary incontinence: systematic review and network meta-analysis of randomised controlled trials
- PMID: 31167796
- PMCID: PMC6549286
- DOI: 10.1136/bmj.l1842
Surgical interventions for women with stress urinary incontinence: systematic review and network meta-analysis of randomised controlled trials
Abstract
Objectives: To compare the effectiveness and safety of surgical interventions for women with stress urinary incontinence.
Design: Systematic review and network meta-analysis.
Eligibility criteria for selecting studies: Randomised controlled trials evaluating surgical interventions for the treatment of stress urinary incontinence in women.
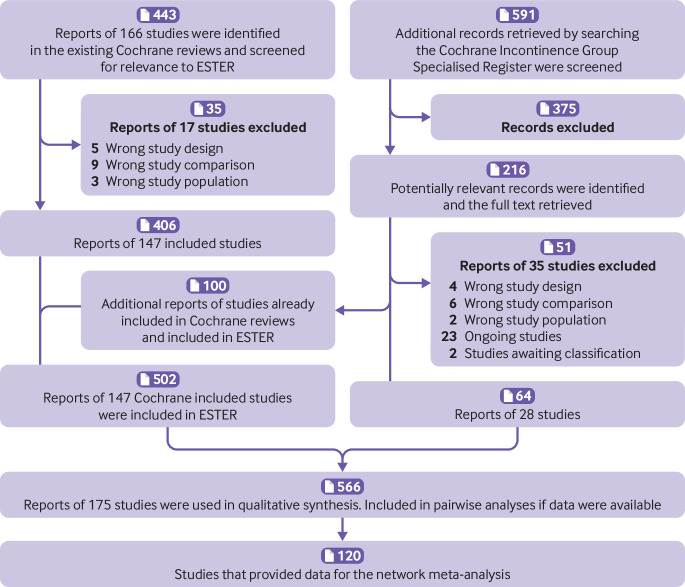
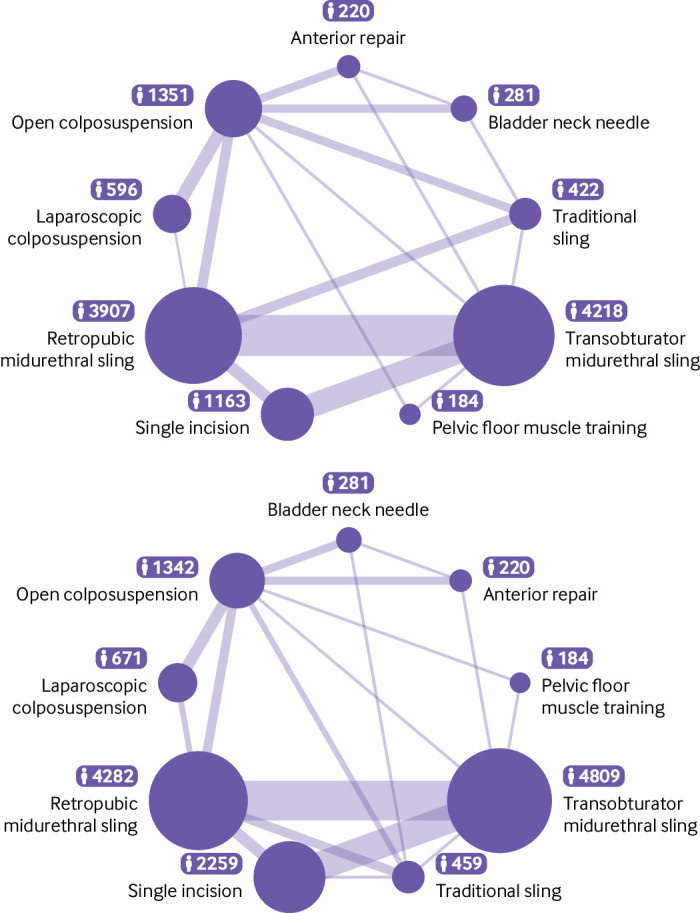
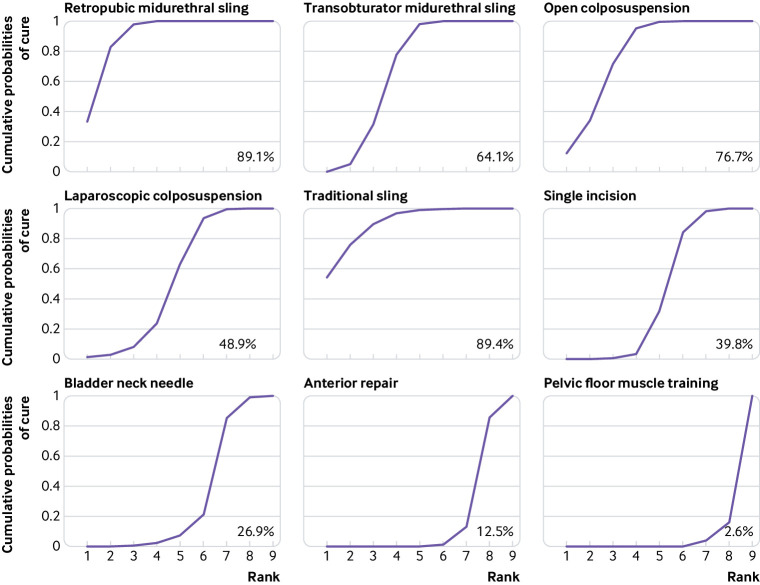
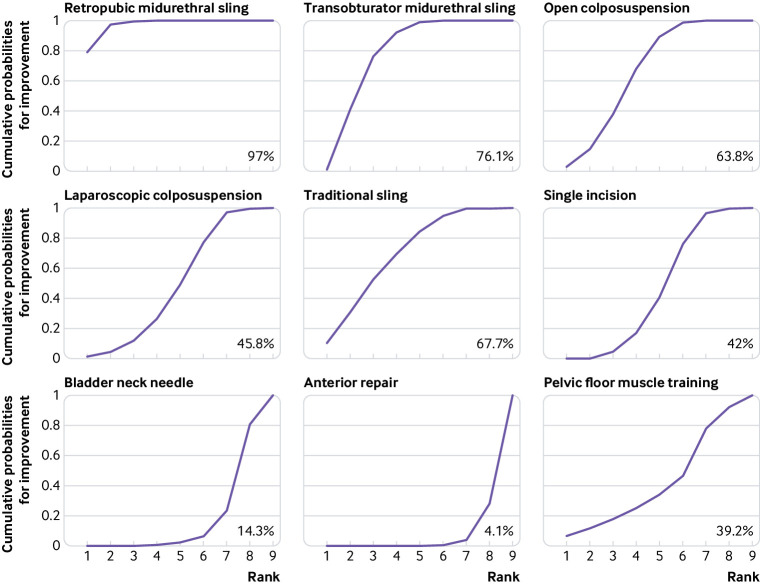
Methods: Identification of relevant randomised controlled trials from Cochrane reviews and the Cochrane Incontinence Specialised Register (searched May 2017), which contains trials identified from the Cochrane Central Register of Controlled Trials (CENTRAL), Medline, Medline In-Process, Medline Epub Ahead of Print, CINAHL, ClinicalTrials.gov, and WHO ICTRP. The reference lists of relevant articles were also searched. Primary outcomes were "cure" and "improvement" at 12 months, analysed by means of network meta-analyses, with results presented as the surface under the cumulative ranking curve (SUCRA). Adverse events were analysed using pairwise meta-analyses. Risk of bias was assessed using the Cochrane risk of bias tool. The quality of evidence for network meta-analysis was assessed using the GRADE approach.
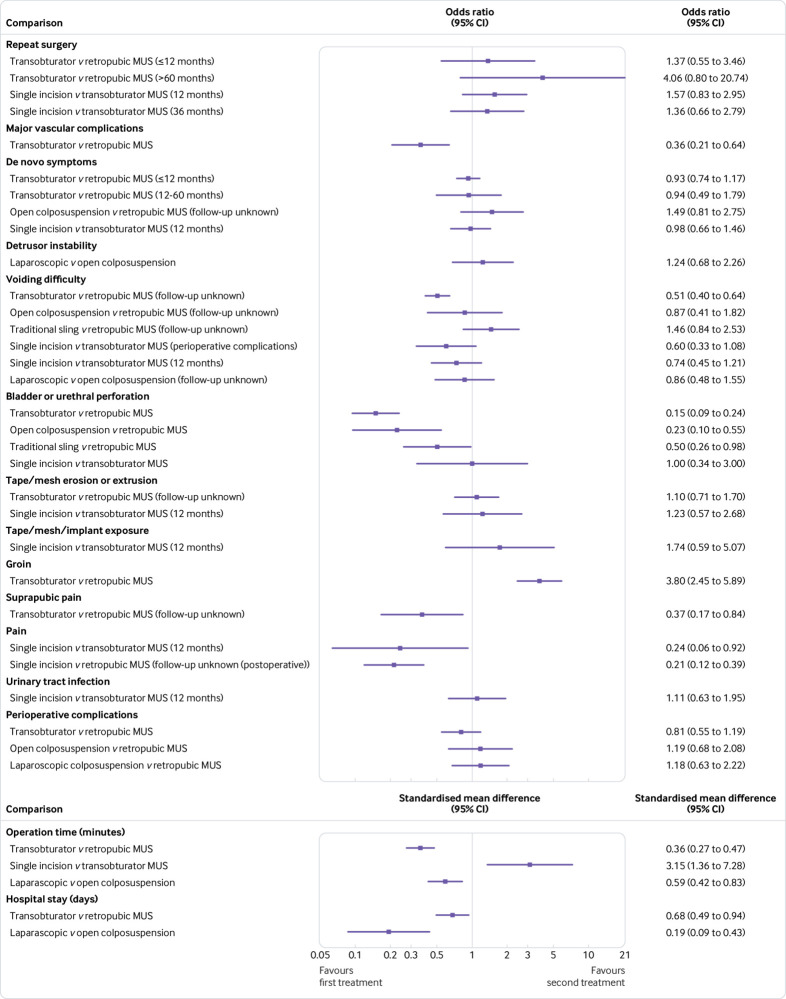
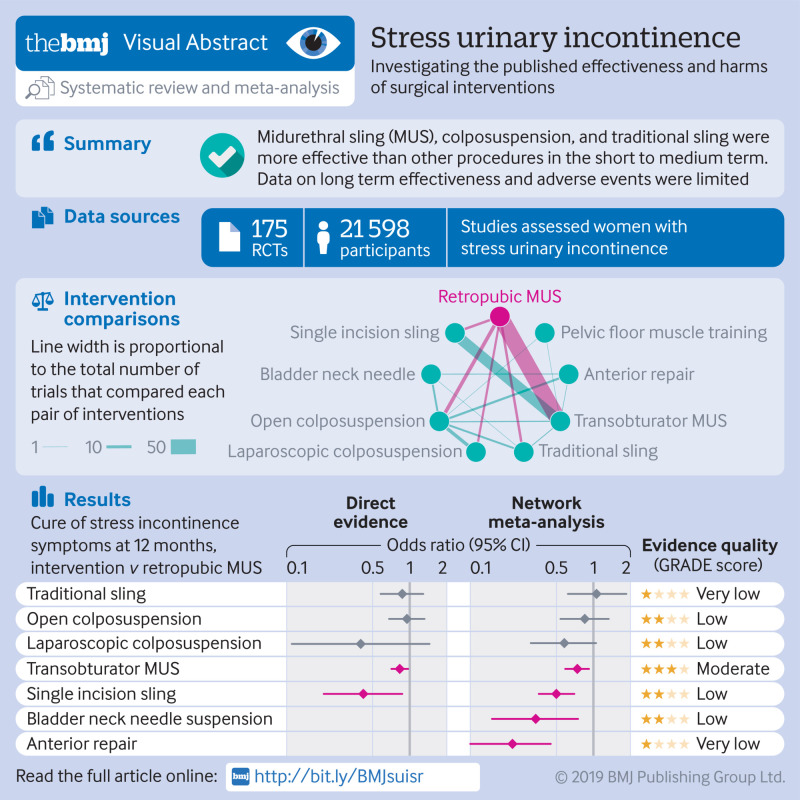
Results: 175 randomised controlled trials assessing a total of 21 598 women were included. Most studies had high or unclear risk across all risk of bias domains. Network meta-analyses were based on data from 105 trials that reported cure and 120 trials that reported improvement of incontinence symptoms. Results showed that the interventions with highest cure rates were traditional sling, retropubic midurethral sling (MUS), open colposuspension, and transobturator MUS, with rankings of 89.4%, 89.1%, 76.7%, and 64.1%, respectively. Compared with retropubic MUS, the odds ratio of cure for traditional sling was 1.06 (95% credible interval 0.62 to 1.85), for open colposuspension was 0.85 (0.54 to 1.33), and for transobtrurator MUS was 0.74 (0.59 to 0.92). Women were also more likely to experience an improvement in their incontinence symptoms after receiving retropubic MUS or transobturator MUS compared with other surgical procedures. In particular, compared with retropubic MUS, the odds ratio of improvement for transobturator MUS was 0.76 (95% credible interval 0.59 to 0.98), for traditional sling was 0.69 (0.39 to 1.26), and for open colposuspension was 0.65 (0.41 to 1.02). Quality of evidence was moderate for retropubic MUS versus transobturator MUS and low or very low for retropubic MUS versus the other two interventions. Data on adverse events were available mainly for mesh procedures, indicating a higher rate of repeat surgery and groin pain but a lower rate of suprapubic pain, vascular complications, bladder or urethral perforation, and voiding difficulties after transobturator MUS compared with retropubic MUS. Data on adverse events for non-MUS procedures were sparse and showed wide confidence intervals. Long term data were limited.
Conclusions: Retropubic MUS, transobturator MUS, traditional sling, and open colposuspension are more effective than other procedures for stress urinary incontinence in the short to medium term. Data on long term effectiveness and adverse events are, however, limited, especially around the comparative adverse events profiles of MUS and non-MUS procedures. A better understanding of complications after surgery for stress urinary incontinence is imperative.
Systematic review registration: PROSPERO CRD42016049339.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; LV reports grants from the NIHR systematic reviews funding stream outside the submitted work and is a member of funding panel NIHR HTA CET panel until march 2018 and coordinating editor of the Cochrane Incontinence Group; AM was a paid speaker for Astellas, SEP Pharma, Boston Scientific, and Atlantic; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Surgical interventions for stress urinary incontinence.BMJ. 2019 Jun 5;365:l2350. doi: 10.1136/bmj.l2350. BMJ. 2019. PMID: 31167751 No abstract available.
References
-
- Milsom I, Altman D, Cartwright R, et al. Epidemiology of urinary incontinence (UI) and other lower urinary tract symptoms (LUTS), pelvic organ prolapse (POP) and anal incontinence (AI). In: Abrams P, Cardozo L, Wagg A, Wein A, eds. Incontinence: 6th International Consultation on Incontinence, Tokyo, September 2016. 6th ed. International Continence Society (ICS) and International Consultation on Urological Diseases (ICUD) 2017:1-141.
-
- Fultz NH, Burgio K, Diokno AC, Kinchen KS, Obenchain R, Bump RC. Burden of stress urinary incontinence for community-dwelling women. Am J Obstet Gynecol 2003;189:1275-82. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical