

Modulation of cytokine patterns and microbiome during pregnancy in IBD
- PMID: 31167813
- PMCID: PMC7034354
- DOI: 10.1136/gutjnl-2019-318263
Modulation of cytokine patterns and microbiome during pregnancy in IBD
Abstract
Objective: Pregnancy may affect the disease course of IBD. Both pregnancy and IBD are associated with altered immunology and intestinal microbiology. However, to what extent immunological and microbial profiles are affected by pregnancy in patients with IBD remains unclear.
Design: Faecal and serum samples were collected from 46 IBD patients (31 Crohn's disease (CD) and 15 UC) and 179 healthy controls during first, second and third trimester of pregnancy, and prepregnancy and postpartum for patients with IBD. Peripheral blood cytokine profiles were determined by ELISA, and microbiome analysis was performed by sequencing the V4 region of the bacterial 16S rRNA gene.
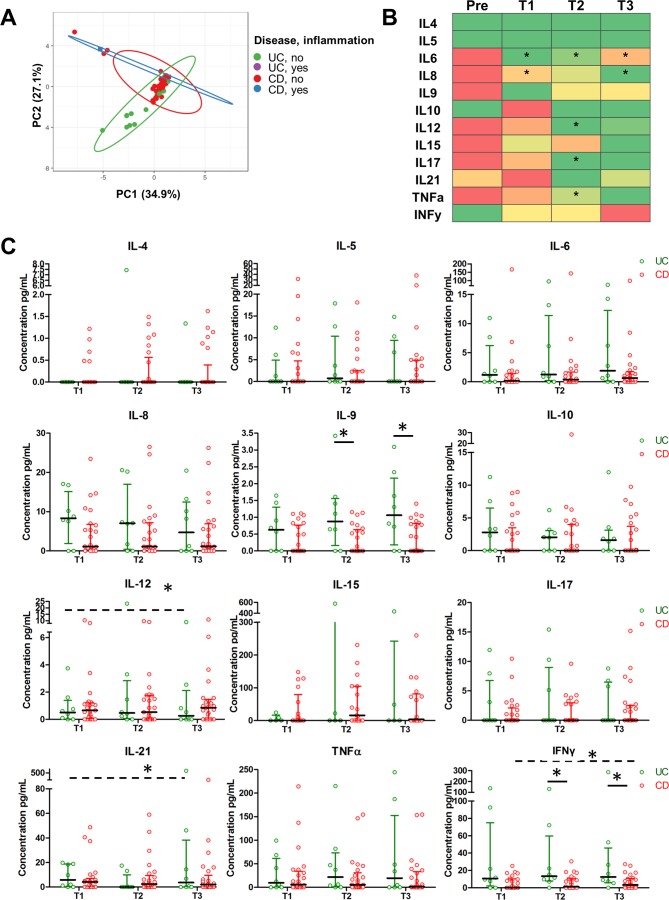
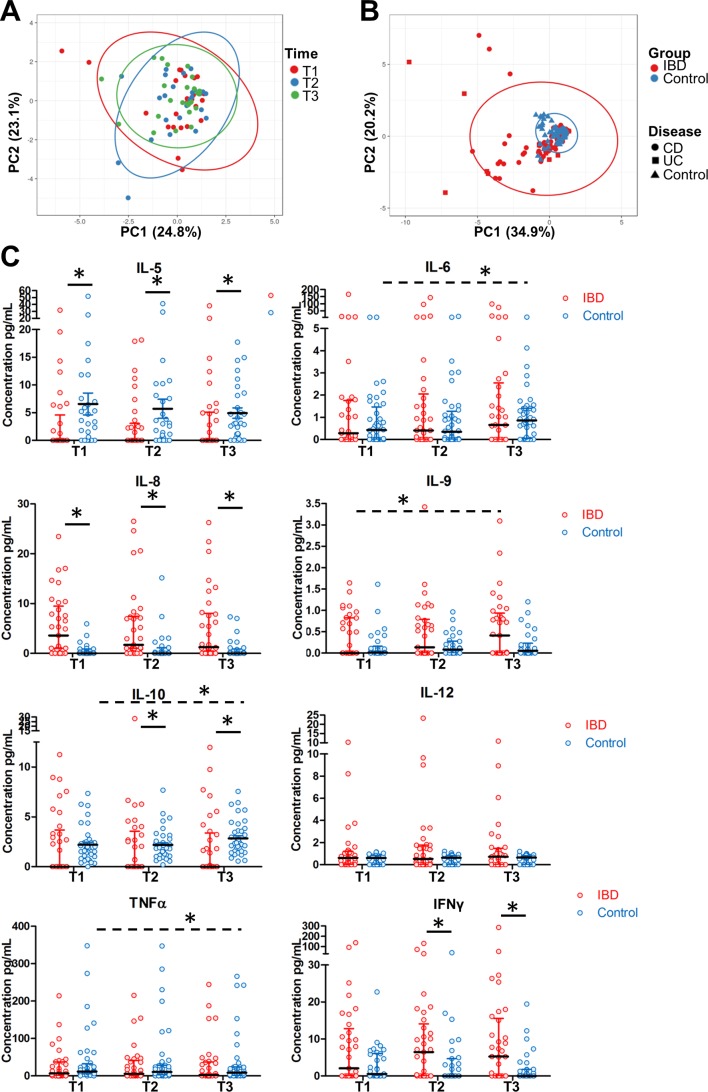
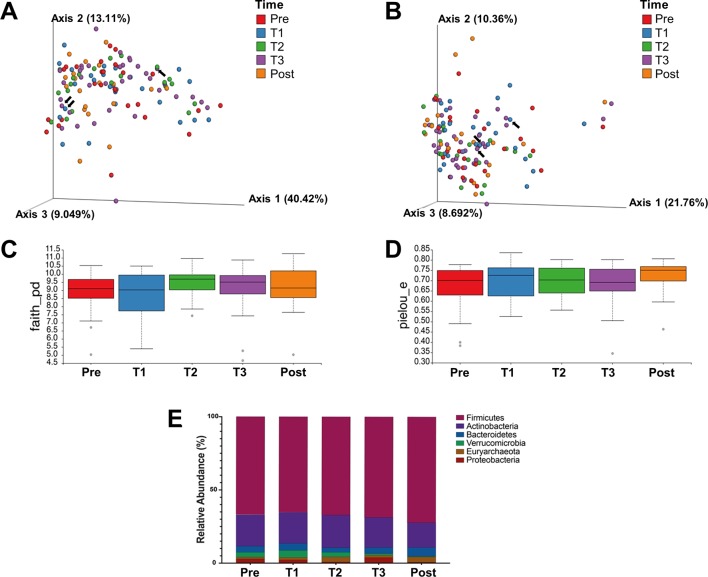
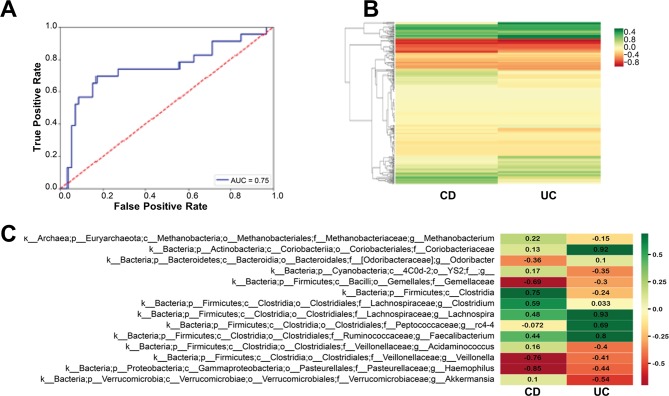
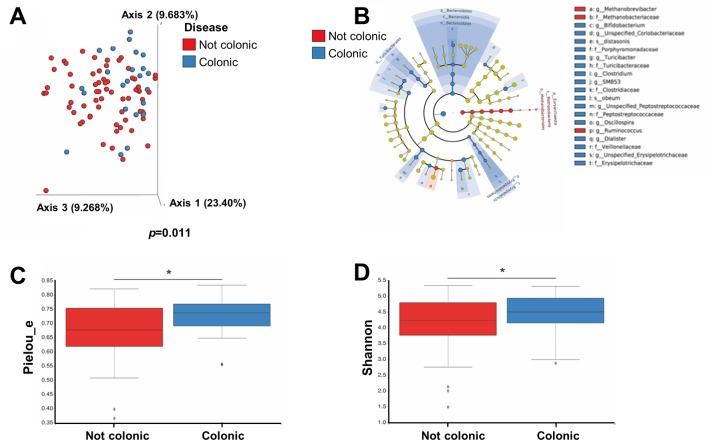
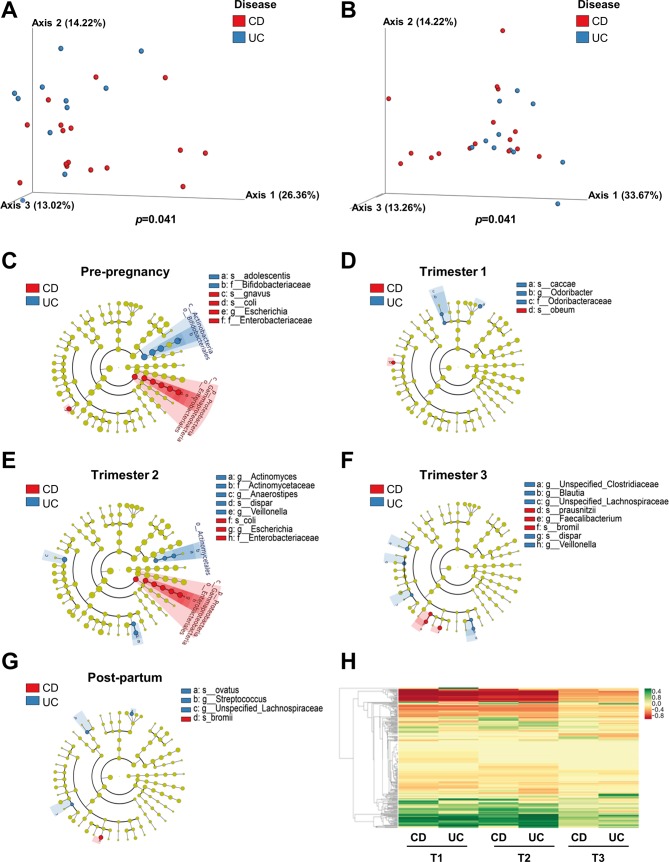
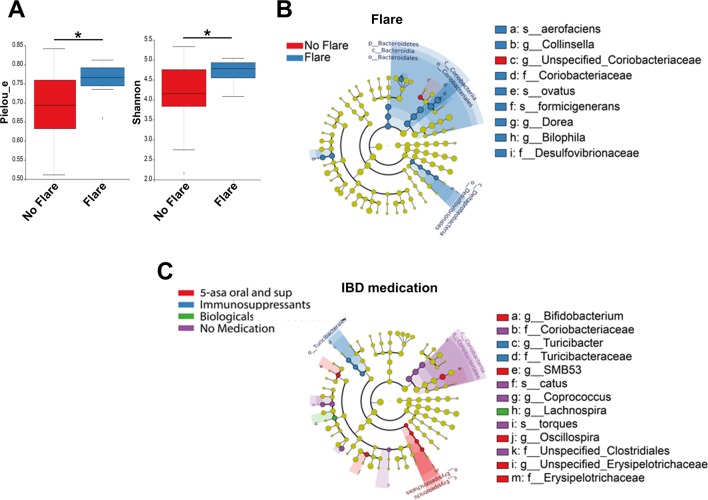
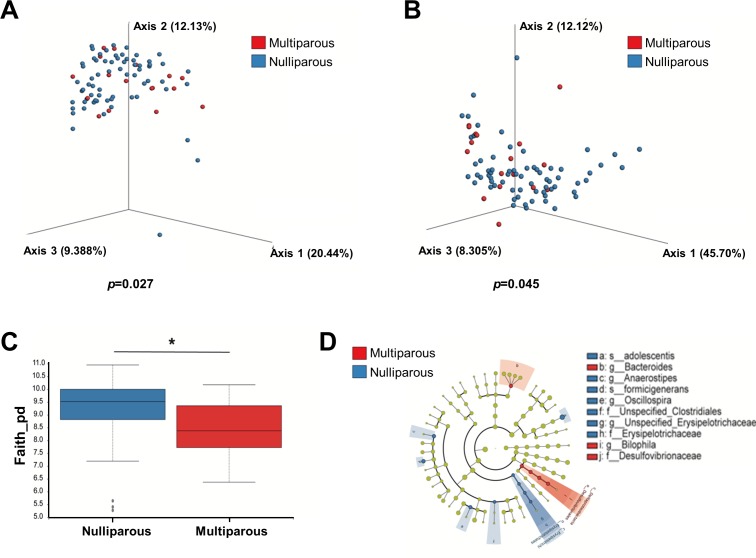
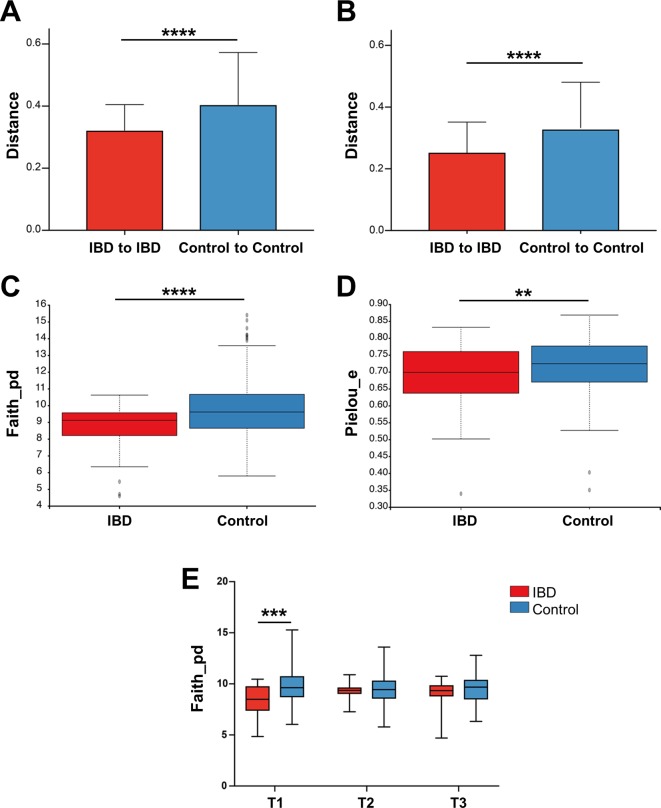
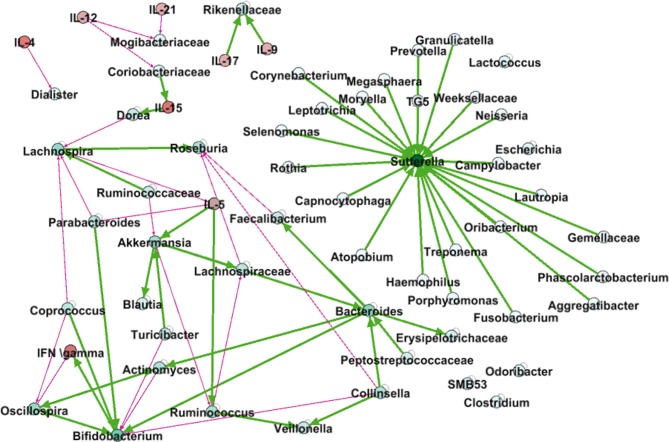
Results: Proinflammatory serum cytokine levels in patients with IBD decrease significantly on conception. Reduced interleukin (IL)-10 and IL-5 levels but increased IL-8 and interferon (IFN)γ levels compared with healthy controls were seen throughout pregnancy, but cytokine patterns remained stable during gestation. Microbial diversity in pregnant patients with IBD was reduced compared with that in healthy women, and significant differences existed between patients with UC and CD in early pregnancy. However, these microbial differences were no longer present during middle and late pregnancy. Dynamic modelling showed considerable interaction between cytokine and microbial composition.
Conclusion: Serum proinflammatory cytokine levels markedly improve on conception in pregnant patients with IBD, and intestinal microbiome diversity of patients with IBD normalises during middle and late pregnancy. We thus conclude that pregnancy is safe and even potentially beneficial for patients with IBD.
Keywords: crohn’s disease; cytokines; inflammatory bowel disease; intestinal microbiology; ulcerative colitis.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Elevated interferon-gamma levels during pregnancy are associated with adverse maternofetal outcomes in IBD.Gut. 2020 Oct;69(10):1895-1897. doi: 10.1136/gutjnl-2019-319656. Epub 2019 Nov 13. Gut. 2020. PMID: 31722975 No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical