

The Influence of Type 2 Diabetes-Associated Factors on Type 1 Diabetes
- PMID: 31167894
- PMCID: PMC6647039
- DOI: 10.2337/dc19-0102
The Influence of Type 2 Diabetes-Associated Factors on Type 1 Diabetes
Abstract
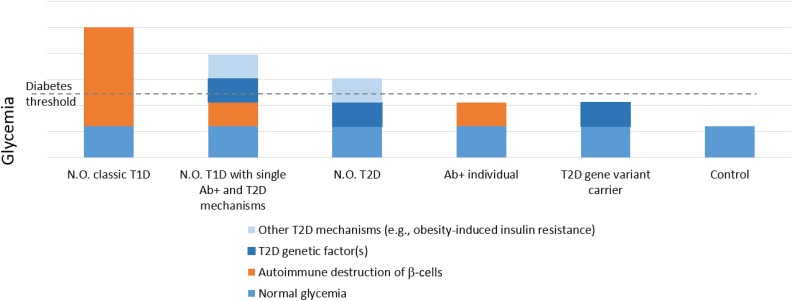
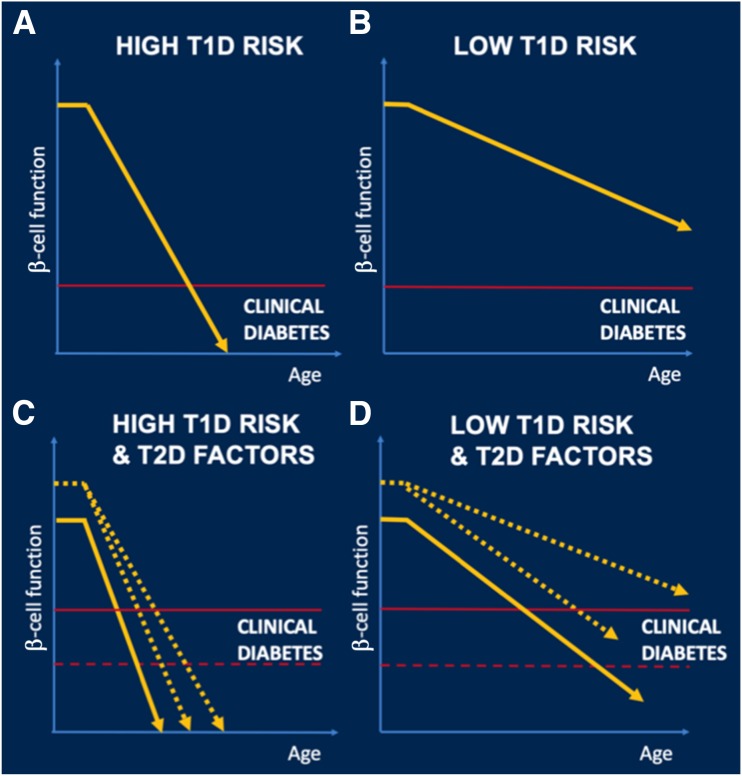
Current efforts to prevent progression from islet autoimmunity to type 1 diabetes largely focus on immunomodulatory approaches. However, emerging data suggest that the development of diabetes in islet autoantibody-positive individuals may also involve factors such as obesity and genetic variants associated with type 2 diabetes, and the influence of these factors increases with age at diagnosis. Although these factors have been linked with metabolic outcomes, particularly through their impact on β-cell function and insulin sensitivity, growing evidence suggests that they might also interact with the immune system to amplify the autoimmune response. The presence of factors shared by both forms of diabetes contributes to disease heterogeneity and thus has important implications. Characteristics that are typically considered to be nonimmune should be incorporated into predictive algorithms that seek to identify at-risk individuals and into the designs of trials for disease prevention. The heterogeneity of diabetes also poses a challenge in diagnostic classification. Finally, after clinically diagnosing type 1 diabetes, addressing nonimmune elements may help to prevent further deterioration of β-cell function and thus improve clinical outcomes. This Perspectives in Care article highlights the role of type 2 diabetes-associated genetic factors (e.g., gene variants at transcription factor 7-like 2 [TCF7L2]) and obesity (via insulin resistance, inflammation, β-cell stress, or all three) in the pathogenesis of type 1 diabetes and their impacts on age at diagnosis. Recognizing that type 1 diabetes might result from the sum of effects from islet autoimmunity and type 2 diabetes-associated factors, their interactions, or both affects disease prediction, prevention, diagnosis, and treatment.
© 2019 by the American Diabetes Association.
Figures

References
-
- Imperatore G, Boyle JP, Thompson TJ, et al. .; SEARCH for Diabetes in Youth Study Group . Projections of type 1 and type 2 diabetes burden in the U.S. population aged <20 years through 2050: dynamic modeling of incidence, mortality, and population growth. Diabetes Care 2012;35:2515–2520 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
