

Therapeutic effect of Anakinra in the relapsing chronic phase of febrile infection-related epilepsy syndrome
- PMID: 31168503
- PMCID: PMC6546072
- DOI: 10.1002/epi4.12317
Therapeutic effect of Anakinra in the relapsing chronic phase of febrile infection-related epilepsy syndrome
Abstract
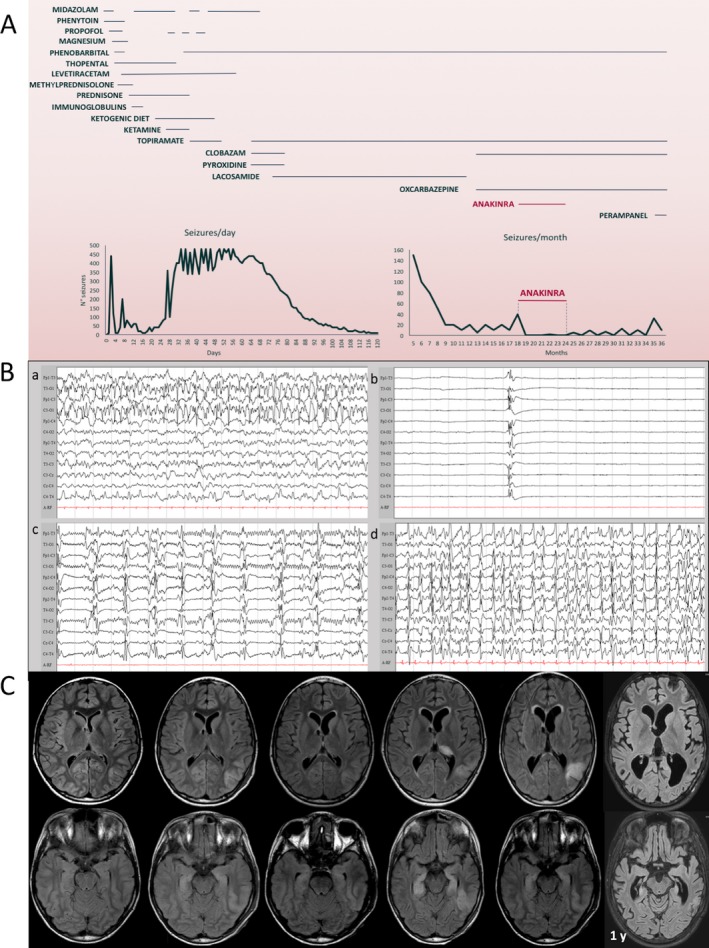
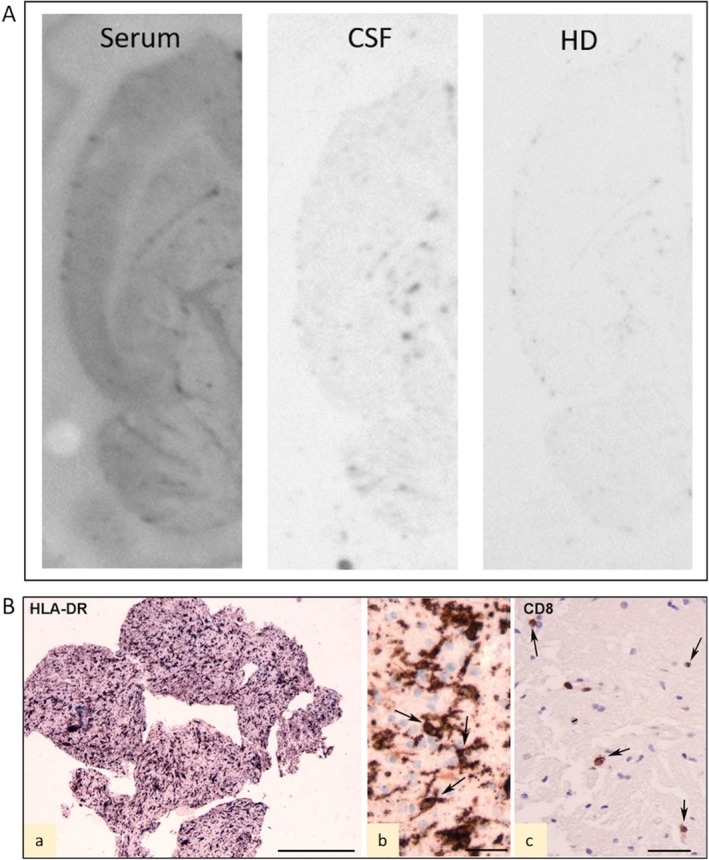
Febrile infection-related epilepsy syndrome (FIRES) is a severe epileptic encephalopathy with presumed inflammatory origin and lacking effective treatments. Anakinra is the human recombinant interleukin 1 receptor antagonist clinically used in autoinflammatory or autoimmune conditions. We report a case of FIRES for which the spatial and temporal match between electroencephalography (EEG) and magnetic resonance imaging (MRI) focal alterations provides support for the detrimental synergic interplay between seizures and inflammation that may evolve to permanent focal lesions and progressive brain atrophy in weeks to months. Brain biopsy showed aspects of chronic neuroinflammation with scarce parenchymal lymphocytes. We report the novel evidence that anakinra reduces the relapse of highly recurrent refractory seizures at 1.5 years after FIRES onset. Our evidence, together with previously reported therapeutic effects of anakinra administered since the first days of disease onset, support the hypothesis that interleukin 1β and inflammation-related factors play a crucial role in seizure recurrence in both the acute and chronic stages of the disease.
Keywords: IL‐1β; epileptic encephalopathy; febrile infection–related epilepsy syndrome; neuroinflammation.
Conflict of interest statement
None of the authors has any conflict of interest to disclose. All co‐authors have been substantially involved in the study and/or the preparation of the manuscript; no undisclosed groups or persons have had a primary role in the study and/or in manuscript preparation. All co‐authors have seen and approved the submitted version of the paper and accept responsibility for its content. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Figures
References
-
- Hirsch LJ, Gaspard N, van Baalen A, Nabbout R, Demeret S, Loddenkemper T, et al. Proposed consensus definitions for new‐onset refractory status epilepticus (NORSE), febrile infection‐related epilepsy syndrome (FIRES), and related conditions. Epilepsia 2018;59:739–744. - PubMed
-
- Vezzani A, Maroso M, Balosso S, Sanchez MA, Bartfai T. IL‐1 receptor/Toll‐like receptor signaling in infection, inflammation, stress and neurodegeneration couples hyperexcitability and seizures. Brain Behav Immun 2011;25:1281–1289. - PubMed
-
- Jyonouchi H, Geng L. Intractable Epilepsy (IE) and Responses to Anakinra, a Human Recombinant IL‐1 Receptor Antagonist (IL‐1Ra): case Reports. J Clin Cell Immunol 2016;7:456–460.
