

PGAM5 is a key driver of mitochondrial dysfunction in experimental lung fibrosis
- PMID: 31168659
- PMCID: PMC11105634
- DOI: 10.1007/s00018-019-03133-1
PGAM5 is a key driver of mitochondrial dysfunction in experimental lung fibrosis
Abstract
Rationale: Mitochondrial homeostasis has recently emerged as a focal point in the pathophysiology of idiopathic pulmonary fibrosis (IPF), but conflicting data have been reported regarding its regulation. We speculated that phosphoglycerate mutase family member 5 (PGAM5), a mitochondrial protein at the intersection of multiple cell death and mitochondrial turnover pathways, might be involved in the pathogenesis of IPF.
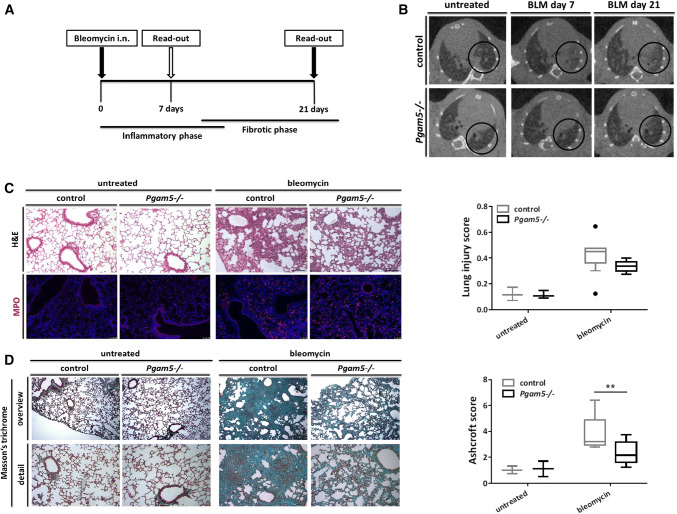
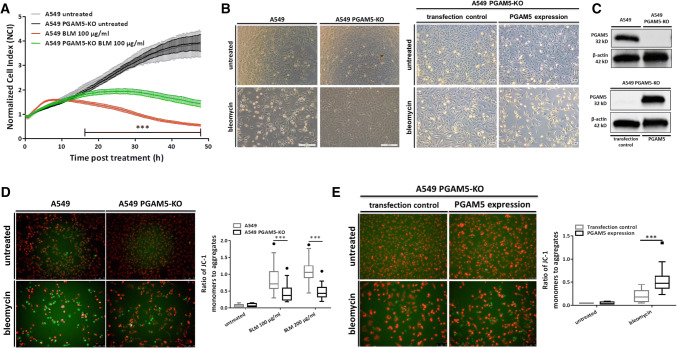
Methods: PGAM5-deficient mice and human pulmonary epithelial cells were analyzed comparatively with PGAM5-proficient controls in a bleomycin-based model of pulmonary fibrogenesis. Mitochondria were visualized by confocal and transmission electron microscopy. Mitochondrial homeostasis was assessed using JC1 (ΔΨ) and flow cytometry.
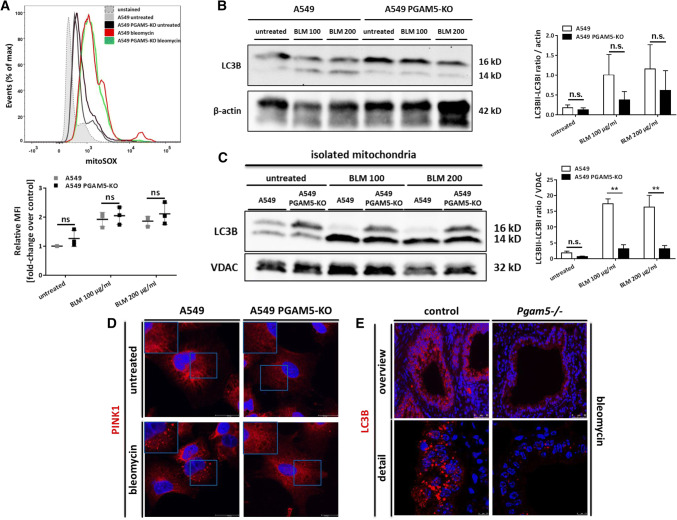
Results: PGAM5 plays an important role in pulmonary fibrogenesis. Pgam5-/- mice displayed significantly attenuated lung fibrosis compared to controls. Complementary, in vitro studies demonstrated that PGAM5 impaired mitochondrial integrity on a functional and structural level independently of mtROS-production. On a molecular level, reduced mitophagy caused by PGAM5 deficiency improved mitochondrial homeostasis.
Conclusions: Our study identifies PGAM5 as an important regulator of mitochondrial homeostasis in pulmonary fibrosis. Our data further indicate PGAM5-mediated mitophagy itself as a pivotal gateway event in the mediation of self-sustaining mitochondrial damage and membrane depolarization. Our work hereby highlights the importance of mitochondrial dynamics and identifies a potential therapeutic target that warrants further studies. Toxic agents lead to mitochondrial damage resulting in depolarization of the mitochondrial membrane potential (ΔΨ) which is a gateway event for the initiation of PGAM5-mediated mitophagy. PGAM5-mediated mitophagy in turn leads to a self-perpetuating escalation of ΔΨ depolarization. Loss of the mitophagy-based damage-enhancing loop under PGAM5-deficient conditions breaks this vicious cycle, leading to improved mitochondrial homeostasis.
Keywords: Bleomycin; IPF; Mitophagy.
Conflict of interest statement
We, the authors, have no conflicting financial interests.
Figures

References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
